- Home
- Prenatal diagnosis
- Prenatal Diagnosis Techniques
Prenatal Diagnosis Techniques
If we are to perform this series of tests during the course of the pregnancy, we will logically have to employ techniques that will allow us to gain access into the foetus. At present, these techniques are divided into invasive and non-invasive techniques of the foetal space.
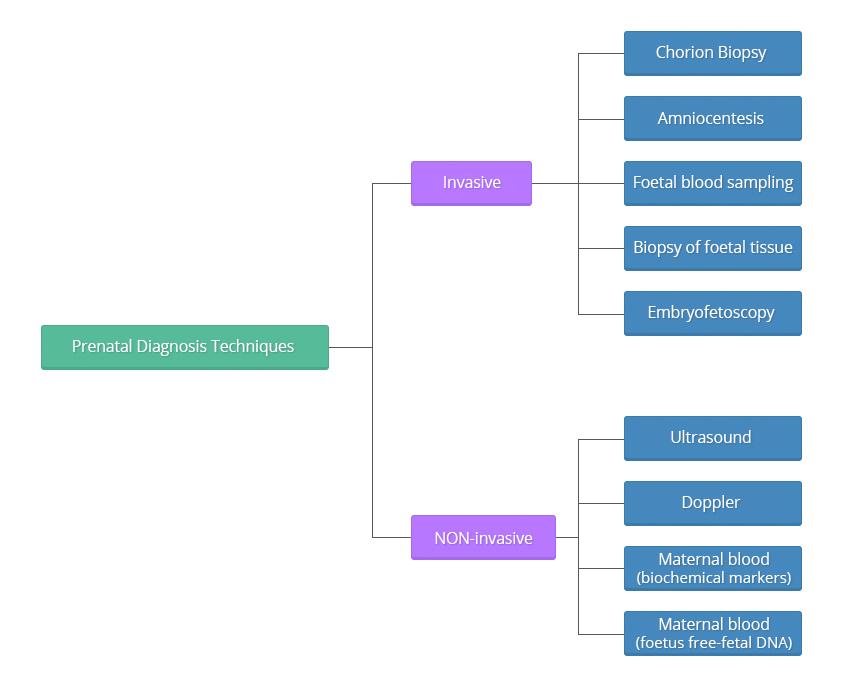
Invasive techniques
Invasive techniques are defined as those that invade or physically enter the foetal space or surroundings, for example, puncturing the amniotic sack to withdraw fluid. These tests must be performed observing very strict sterility measures.
The difference among these techniques is the time or weeks of gestation at which they are performed during the pregnancy; the reliability of the tests, as they all present an error margin (remember that in medicine there is never 0 or 100, we always talk in terms of probability); and the risk of miscarriage, which varies depending on each particular technique.
These techniques should be performed at specific times throughout the gestational period in order to increase the possibility of getting a reliable result while, at the same time, decreasing the risk of miscarriage, and should always be performed under ultrasound guidance.
The adoption of a specific technique will depend on the type of diagnosis required.
In all cases, and whenever possible, the safest technique with the fastest results will be used. For obvious reasons, it is different to inform the patient of a pathological finding at 11 weeks than it is when she is already into her 22 week.
If chromosomal determinations are required, any of these techniques will be appropriate. However, chorionic biopsy and amniocentesis are the most recommendable tests, as they can both be performed early in the pregnancy and provide the greatest experience.
- Chorion Biopsy
Chorion Biopsy
A chorion biopsy is the collection of villi from the chorionic area of the growing placenta. This type of biopsy should always be performed under ultrasound guidance, and may either performed transcervically or transabdominally using a catheter or a clamp appropriate to the gestational age.
The test must be performed after the 11th week of pregnancy to term. If the test if performed before the 10th week, it can lead to abnormalities of the fetal limbs, micrognathia and microglossia. For purposes of prenatal diagnosis of chromosomal defects or inherited diseases for DNA alterations, the optimum gestational age to carry out the procedure is between the 11th and 12th weeks of pregnancy.
Chorionic villi provide excellent material to conduct DNA molecular studies and enzymatic determinations.
The risk of miscarriage due to the technique is unknown, as in this gestational period, many spontaneous abortions occur. It remains unknown whether any of the women who underwent the test would have also ended in miscarriage, should they not had the test. Presently, this risk is estimated about 1%.
Transcervical approach
The catheter is inserted through the vagina and uterine neck into the uterus to the edge of the placenta where the chorionic villi is snipped or suctioned off for diagnosis.
Transabdominal approach
In the transabdominal procedure, a needle is inserted through the abdomen to the edge of the placenta from where the chorionic villi will be obtained.
- Amniocentesis
Amniocentesis
This procedure consists in the extraction of amniotic fluid through a needle that has been inserted transabdominally under ultrasound guidance. For purposes of chromosomal or genetic disorders diagnosis, amniocentesis is habitually performed between the 14th and 20th weeks of pregnancy, (ideally between 15 and 17) obtaining about 15 to 20 ml of amniotic liquid. It has been shown that if the test is performed earlier in the pregnancy, the uterus is not as accessible and the number of foetal cells is scarce, and if performed later in the pregnancy, we run the risk that many of the cells obtained are keratinised and unfeasible for study.
If the test is performed between the 15th and 20th week of pregnancy the risk of spontaneous abortion is less than 1%.
Amniocentesis is also possible at 10-14 weeks of gestation. If the test is performed during these earlier weeks, the risk of spontaneous abortion increases around 2%, and there is a higher incidence of talipes equinovarus (foot abnormality), as well as rupture of the membranes; hence, although technically possible, this procedure is NOT recommended and should only be used in very specific cases and with the patient´s consent.
Complications of amniocentesis:
Spontaneous abortions (miscarriages) = < 1%
Contamination of the amniotic fluid by stem cells = 0.15 – 0.11%.
Loss of amniotic fluid = 1 – 2 %.
Blood loss, with scanty “spotting”, very rare.Complications with amniocentesis are rare under adequate asepsis. However, one of the unlikely complications would be an infection in the mother.
- Foetal blood sampling
Foetal blood sampling
This test obtains foetal blood by direct puncture of the funicular vessels under ultrasound or foetoscopic guidance.
The main indications of this technique include: Rapid assessment of foetal chromosomes (results can be obtained within 24 to 48 hours), immunological assessment of the foetus, and assessment of certain haemopathies or blood disorders.This test is usually performed after the 20th week of pregnancy through delivery. It is not advisable to perform this test in the early stages of pregnancy because blood vessels in the umbilical cord are very small at this stage of development and can get damaged when they are punctured to extract the blood.
Normally between 0.5 and 4 ml of foetal blood are collected. The sample is analysed immediately to make sure it is foetal blood, as the maternal placental blood vessels are in close proximity to where the sample is collected and an error could easily occur.
The risk of spontaneous abortion as a result of the test is approximately 1-3%.
- Biopsy of foetal tissue
Biopsy of foetal tissue
This technique is used to obtain foetal tissues for specific testing or screening, such as skin, liver or muscular biopsies.
As in the previously described techniques, the procedure is always carried out under ultrasound or foetoscopic guidance. - Embryofetoscopy
Embryofetoscopy
Embryofetoscopy consists in the direct visualisation of the embryo or fetus during pregnancy through a device called endoscope or fetoscope.
- When this technique is performed during the first 12 weeks of pregnancy, it is called embryoscopy.
- When performed after the 12th week of pregnancy, it is called fetoscopy.
Embryofetoscopy is used for therapeutic and diagnostic purposes only when it is NOT possible to obtain the same results using ultrasound or ultrasound combined with other prenatal diagnosis techniques such as chorion biopsy, amniocentesis or funiculocentesis, due to the risks involved for both the mother and her unborn child. These risks can include: a 12% risk of miscarriage, bleeding, infection, liquid loss, sensitivisation problems caused by paternal Rh- incompatibility if adequate prevention measures are not taken, and a 47% risk of premature rupture of the membranes.
Consequently, embryofetoscopy should only be carried out in specialised centres with qualified professionals trained in this sort of procedures and with the appropriate equipment (fetoscopes, with specific instruments designed for each task, video cameras, digital cameras, light sources and energy, etc.).
Embryofetoscopy should always be performed under ultrasound guidance.
Diagnostic uses
Embryofetoscopy detects congenital malformations and hereditary diseases which can only be diagnosed by:
- Direct external visualisation, for instance in genodermatosis (hereditary diseases of the skin where molecular biology studies cannot be carried out).
- Morphological visualisation of some external anomalies suspected during the ultrasound examination in the early phases of pregnancy.
Collection of foetal blood samples or amniotic fluid samples.
Administration of drugs or therapeutic agents to the foetus.
Therapeutic uses
Fetoscopy enables us to carry out explorations of the foetus, umbilical cord, placenta or membranes.
Most indications on the foetus are still the subject of research with the hope that the applications will help us to save their lives or prevent irreversible sequelae: shunt placement, in cases of obstructive processes, destructions of amniotic bands, treatment for the premature rupture of membranes, tracheal occlusions for the treatment of diaphragmatic congenital hernias, treatment of sacrococcigeous teratomas, treatment of placental chorioangiomas, cord occlusions to carry out selective feticides in monochorial twins, fulguration of posterior urethral valves in lower urinary obstruction, repair of myelomeningocele, etc…
At present, the main application of this technology for therapeutic aims is applied in the treatment of twin-to-twin transfusion syndrome.
This syndrome is a disease of the placenta that affects mainly about 15% of monochorial twins (foetuses that have evolved from one single ovum and spermatozoon and that share the same placenta) due to the formation of abnormal vascular placental connections between the two twins.
Under normal conditions, each twin has its own balanced circulatory system.
However in this kind of twins is frequently that they establish connections between them. There can be different types of vascular connections: between arteries, between veins or artery-to-vein.
Amongst these connections, artery-to-vein connections can be the most problematic, depending on whether they are balanced or unbalanced.
Balanced connections
Unbalanced connections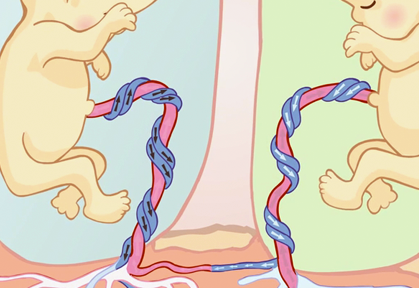
When these connections are balanced, there is no problem (as the blood flow is also in balance and both foetuses are donors and recipient at the same time).
A twin can die prenatally because the recipient foetus has an overloaded circulatory system which can lead, among other complications (polyhydramnios) to heart failure, whereas the donor foetus develops a severe anaemia that prevents growth.
On occasions, if the blood flows in one single direction because it is the blood of one of the twins passing to the other through pathological connections, there is a haemodynamic unbalanced known as twin-to-twin transfusion syndrome. In this instance, one of the foetuses is the donor and the other the recipient.
If the condition is not diagnosed and corrected in time, both foetuses run the risk of dying, either before (prenatally) or after birth (postnatally).
A twin can die postnatally because of premature birth or “prematurity”. Some of those who survive (10%) can develop very serious neurological problems among them brain paralysis.
At the present time, the best treatment consists in the identification and coagulation of the abnormal vascular connections by means of laser endoscopic surgery that blocks the passage of blood from one twin to the other.
NON-Invasive techniques
As regards non-invasive techniques, these procedures do not pose any risk of abortion. Non-invasive diagnostic methods include: Methods that employ ultrasonic waves such as the ULTRASOUND and the DOPPLER examination, which can be safely used at any time during the pregnancy through delivery. And blood chemistry tests using MATERNAL BLOOD (maternal blood testing) during the first and second trimesters of the pregnancy.
- Ultrasound
Ultrasound
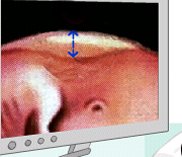
An ULTRASOUND or echography uses ultrasonography or “sound waves” as a diagnostic tool. An ultrasound sends waves to the foetus that bounce off internal foetal structures (thereby its name “echo”). It allows visualisation of the foetus in a TV-like viewing screen, providing internal as well as external images of the foetus. Internal and external malformations can be diagnosed based on different tissue densities. It works in the same way as radars in air traffic control or marine navigation.
Given the constant progress being made in this field, it is now possible to explore the foetus in a bi-dimensional plane (2D) or in a three-dimensional plane, either in a static (3D) or in movement (4D). The use of this technique requires:- Highly qualified professionals in this field.
- The use of devices equipped with the latest technology and approved by the competent regulatory authorities.
View 2D ultrasound on Youtube View 3D ultrasound on Youtube View 4D ultrasound on Youtube
 Occasionally, it is necessary to employ other diagnostic techniques to complement the ultrasound diagnosis, such as magnetic nuclear resonance. This technique employs state of the art devices for rapid image acquisition and storage (which is ideal for the foetus as it is in constant motion within the womb) and allows us to perform an anatomical foetal tracing, which is very useful to confirm certain pathological conditions of the central nervous system, as well as other thoracic and renal pathologies. This image shows a foetus with a diaphragmatic hernia; this means that its lung capacity is partly occupied by intestinal content.
Occasionally, it is necessary to employ other diagnostic techniques to complement the ultrasound diagnosis, such as magnetic nuclear resonance. This technique employs state of the art devices for rapid image acquisition and storage (which is ideal for the foetus as it is in constant motion within the womb) and allows us to perform an anatomical foetal tracing, which is very useful to confirm certain pathological conditions of the central nervous system, as well as other thoracic and renal pathologies. This image shows a foetus with a diaphragmatic hernia; this means that its lung capacity is partly occupied by intestinal content.
The series of images shown next correspond to a girl’s face with a mouth tumour (epulis) studied using the previously mentioned techniques.
Conventional ultrasound 
Three-dimensional ultrasound 
Magnetic resonance You can see some images of the newborn girl before and after the tumor removal (epulis). Viewer discretion is advised. View surgery pictures 
Girl picture at one month oldThis association of techniques for certain malformations permits us to suspect the aetiology of these malformations, to determine the type of tissue or tissues involved; and to establish the prognosis of the alteration, should it be left to run its natural course, and based on this, to determine:
- What is the best time to induce labor, as some malformations can compromise the life of the child, or if allowed to overgrow they may produce irreversible lesions in the actual organ or surrounding tissues.
- To plan the birth, that is a vaginal delivery or by means of a C-section.
- To have a perinatology and/or surgical team ready at the Labour and Delivery Room for the immediate care of the newborn.
- Doppler
Doppler
A DOPPLER also uses sound waves as a diagnostic tool, but the waves are sent to the foetal blood instead, allowing us to study the placental flow and the foetal circulatory system. By assessing the path followed by the blood in the organs, malformations or alterations of the circulatory system can be easily diagnosed.
- Maternal blood (biochemical markers)
Maternal blood tests
 In these tests, a sample of the maternal blood is taken during pregnancy to quantify a series of substances segregated by the foetus or placenta. This assessment allows us to identify pregnant women who are at risk of having a baby affected with some type of chromosomal condition (trisomy 13, 18, 21 (this latter one is also known as Down’s syndrome or mongolism), Turner’s syndrome (45, X), triploidy, etc. Or certain malformations, among these defects of the neural tube such as spina bifida (also known as open dorsal spine) and anencephaly.
In these tests, a sample of the maternal blood is taken during pregnancy to quantify a series of substances segregated by the foetus or placenta. This assessment allows us to identify pregnant women who are at risk of having a baby affected with some type of chromosomal condition (trisomy 13, 18, 21 (this latter one is also known as Down’s syndrome or mongolism), Turner’s syndrome (45, X), triploidy, etc. Or certain malformations, among these defects of the neural tube such as spina bifida (also known as open dorsal spine) and anencephaly.
These test should be performed at specific weeks of pregnancy because their values change as the pregnancy progresses and if these tests are performed outside these times, they may no longer be of informative value. At present, these tests are performed during the first and second trimesters, and, among all the available markers, the most commonly tested ones are:
- During the first trimester (8 to 13 weeks of pregnancy, ideally during the 10th week).
- B-hCG (free beta fraction of human chorionic gonadotropin) and PAPP-A (pregnancy associated plasma protein A) levels are determined.
- During the second trimester (14 to 20 weeks of pregnancy, ideally during the 16th week): this test can be of three different types depending on whether two, three or four substances are measured; in the first case we will be talking about double screening, in the second case, a triple screening and in the third case, a quadruple screening.
- Double screening: This test measures the concentrations of two substances: alpha-fetoprotein AFP and hCG (total or free-beta).
- Triple screening: This test measures the concentrations of three substances, namely AFP, hCG (total or free-beta), non-conjugated estriol uE3.
- Quadruple test: This test measures the concentrations of four substances AFP, hCG (total or free beta), uE3 and inhibin-A.
Before reporting the results, the laboratory should assess the results obtained taking into account the mother’s age and a series of factors that have the capacity to modify the levels of these substances such as the mother’s weight, the race, smoking, insulin-dependent diabetes, the number of foetuses carried in the pregnancy (twins, triples, etc.)
At present, these biochemical tests are complemented with ultrasound studies to increase their detection rate. Subsequently, and taking into account these two results (biochemical + ultrasound examinations), together with the clinical history and the mother’s age, the individual risk is calculated for each individual patient. It must be made clear that if the test yields an abnormal result, it does NOT mean that a chromosomal alteration has been diagnosed, given that these tests are not of diagnostic value.
These tests only alert us about the POSSIBILITY of existence of some type of alteration. Consequently, once the results become available, the physician will determine whether further tests are necessary (chorion biopsy, amniocentesis, etc.).Now, let’s focus on the ECHOGRAPHIC MARKERS. Echographic markers are assessed when fetal echographic examinations are carried out during the first and second trimester of pregnancy.
First trimester
There are several ultrasound markers used to detect chromosomal disorders during the FIRST TRIMESTER as each abnormality follows its own syndromic pattern of detectable alterations (megalocystis, single umbilical artery, crown-rump length, etc.). Nevertheless, given its great importance in the detection of the most frequently occurring chromosomal alterations (trisomy 13, 18, 21 and Turner’s syndrome (45,X), we will rule out the following.
Nuchal translucency (NT)
An ultrasound marker consisting in the measurement of the physiological accumulation of liquid in the foetal neck while pregnancy is between 8 to 14 weeks.

This is a pathological translucency. The risk of a chromosomal defect starts after a given thickness.

This is a normal translucence
Assessment of presence/ absence of foetal nasal bone
The nasal bone is commonly visualised during an ultrsound examination. Nonetheless, given that size of the nose is an thnic feature, it may be not possible to visualise this structure in normal foetuses. The incidence of this occurrence is 1% for Caucasians, 10% for African-Caribbean, and 7% for Asiatics.
 Presence of the nasal bone (please observe the two whitish structures making a = sign and the tip of the nose at the most prominent end)
Presence of the nasal bone (please observe the two whitish structures making a = sign and the tip of the nose at the most prominent end)
Absence of the nasal bone (a whitish structure which is the tip of nose is only observed)
On the other hand, the nasal bone is absent in 60-70% of foetuses with trisomy 21, in approximately 50% of the foetuses with trisomy 18 and in 30% of foetuses with trisomy 13.
A Doppler study of blood vessels and the foetal heart rate
The ductus venosus study (blood vessel that transports most of the venous blood from the placenta to the heart) is especially sensitive, given that when it is affected, we should suspect the presence of certain chromosomal alterations as well as cardiac malformations.
Normal ductus venosus
Pathological ductus venosus: Please notice that the images transmitted by the blood flow wave are different to those of a normal pattern
Doppler assessment of tricuspid insufficiency
Tricuspid insufficiency occurs in 65% of foetuses with trisomy 21 and in 6% of foetuses who have healthy chromosomes.
Assessment of the craniomaxillofacial angle
An upper facial angle of 85º is present in 65% of cases of foetuses with trisomy 21 and in 5% of chromosomically normal foetuses. The most commonly used echographic marker in the first trimester nuchal translucency, whereas the rest of markers are usually used when nuchal translucency results reach borderline values or pregnancies at very high risk of chromosome pathology. Just so that you get an idea, the screening for trisomy 21 in the first trimester (which combines ultrasound for nuchal translucency and nasal bone + the determination of free Beta-hCG and PAPP-A in maternal blood) allows the clinician to potentially identify over 90% of pregnancies with this syndrom, with a false positive rate of 2,5%.
Second trimester
Several echographic markers are used to detect cromosopathies during the SECOND TRIMESTER and their reliability to calculate the risk of chromosomal alterations is different from each marker.
The assessment of echographic markers i s perfomed between weeks 18 and 22. The most commonly performed test are: the asessment of nuchal fold (measurement of the foetus’s neck thickness which should not generally exceed 6 mm.) and the assessment of cysts in the choroid plexuses being the most commonly performed. Apart from the different types of fetal malformations that might be detected, these malformations, when assessed as a whole, make us suspect specific chromosomal pathologies in certain cases. When a malformation is found during the ultrasound examination, the ultrasound specialist will take a closer, more thorough look into the foetal anatomy in an attempt to find any other accompanying malformations.
It should be made clear that this type of ultrasound examinations should only be carried out by qualified and trained professionals and that the determination of maternal serum markers should only be carried out by duly accredited laboratories.
And please, regardeless of all the information you get, keep in mind that all the information is merely informative and should be correctly interpreted. It is very important that you do not get alarmed and that before taking any decision, you seek the advice of your gynaecologist. If your doctor deems it necessary, he will refer you to a Genetics department, where your particular case will be assessed and all your questions and doubts will be answered, together with a set of instructions to follow in your particular case.
- During the first trimester (8 to 13 weeks of pregnancy, ideally during the 10th week).



{kind=link}

If you click on the different buttons appearing in the previous illustration, you will find information, animations and links relating to the subject matters. This information will help you understand what each of the techniques is and what it is used for. Most likely, you are asking yourself the following questions:
Related questions
- What types of prenatal screening are there?Several different screening modalities can be employed depending on the pathology to be detected, the time of pregnancy in which these modalities might be used and markers to be identified, as follows:
- Screening for chromosomal alterations
- Screening of neural tube defects
- Screening for cardiopathies
- Screening in multiple pregnancies
Screening for chromosomal alterations
This screening test is performed to assess the probability of a childbearing woman in an on-going pregnancy to carry a foetus with a chromosomal alteration. The most frequent and commonly assessed chromosome pathology by means of screening methods is trisomy 21, although trisomy 18 and 13 can also be determined. Depending on the markers used, Turner’s syndrome can also be detected (45, XO). The risk of a pregnant woman to be carrying a fetus with trisomy 21, 18 or 13 is related to her age. This refers to the so-called ‘a-priori’ risk for maternal age. Screening methods are based on a modification of the ‘a-priori risk’ for maternal age based on the results yielded by the combination of the markers analysed. If the analysed markers are normal, the final risk will decrease and if the markers are abnormal, such risk will increase. This probability or risk is calculated using computer programs that employ mathematical formulas published in the scientific literature. However, each program should have its own reference values mainly based on the laboratory techniques used.
Consequently, when different laboratories perform such tests, it is possible for the same pregnant woman, in an identical gestation, and with the same markers analysed, to obtain slightly different results when calculating the probability of foetus being affected with a chromosomal alteration or when calculating the risk. An established cut-off level in the screening tests is used to classify the screened patients into two groups. Such classification is usually expressed as a fraction of 1 amongst X (for instance 1:270), reflecting the way in which the cut-off level is applied whereby all patients below the 1:270 mark will run a higher risk of having an affected child (for instance 1:190) whilst all patients falling above the 1:270 mark will be considered low-risk (for instance 1:300). The perception of risk is very subjective and can differ greatly amongst different individuals. However, the aim of population screening programmes financed by the public health system is to attempt to achieve the maximum possible efficacy of the screening method used in order to obtain a cut-off point that optimises detection and that decreases the number of false positives. For standard screening tests, this cut-off point currently stands between 1:250 and 1:350. Different types of screening exist, depending on which markers are used and the time of the pregnancy when the screening is carried out.
First trimester
Biochemestry screening: this screening method analyses maternal blood between the 8 and 13 weeks of pregnancy and determines the values of certain substances, of which the most important are: B-hCGB-hCG (free beta fraction or total human chorionic gonadotropin) and PAPP-A (pregnancy associated plasma protein A). Nonetheless, other markers, which will probably be very useful during the first trimester of pregnancy, are currently under study. Screening based of two single markers is not commonly performed in the first trimester.
Echographic or ultrasound screening: this screening consists in the determination of echografic makers, of which the most commonly used at present during the first trimester are:
Nuchal translucency or nuchal fold scan (NT) is an echographic marker used in the first trimester (when you are from 8 to 14 weeks pregnant) that measures the thickness of the physiological liquid accumulated in the baby’s neck using ultrasound. The best time to do the scan is when the length from crown to rump (CRL) of the foetus is between 45 and 85 mm, which usually occur between the 11 and 14th weeks of gestation. Nuchal translucency thickness increases with the gestational age, and thus the importance of the measured thickness is in relation to foetal length. In general terms, a nuchal translucency measurement below 3 mm is considered normal in most cases.
Other echographic or ultrasound markers used include:
Assessment of the presence or absence of the nasal bone of the foetus. The face of individuals with Down syndrome is flattened and their nose is small. This might be attributed to a delay in the development of the nasal bone. Upon echographic exploration this echographic alteration manifests as the non-visualisation of the nasal bone in the first trimester or a smaller size than that expected for the second trimester. The nasal bone is absent in 60-70% of the foetuses affected with trisomy 21, in approximately 50% of foetuses with trisomy 18 and in 30% of foetuses with trisomy 13. The size of the nose is an ethnical feature and because of this in normal foetuses, the nasal bone might be absent in 1% of Caucasians, in 10% of Afro-Caribbean and in 7% of Asiatics.
Presence of the nasal bone (please observe the two whitish structures making a = sign and the tip of the nose at the most prominent end)Absence of the nasal bone (a whitish structure which is the tip of nose is only observed)
The most commonly used echographic marker in the first trimester is nuchal translucency, whereas the rest of markers are usually used as second-line markers when nuchal translucency results reach borderline values or pregnancies at very high risk of chromosome pathology.
Ductus venous Doppler examination. The ductus venous is a vessel that transports blood from the placenta to the foetal heart; some sort of chromosomal alteration is suspected when the flow wave of this vessel is pathological.
Doppler assessment of tricuspid insufficiency: Tricuspid insufficiency occurs in 65% of foetuses with trisomy 21 and in 6% of foetuses who have healthy chromosomes.
Assessment of the craniomaxillofacial angle: An upper facial angle of 85º is present in 65% of cases of foetuses with trisomy 21 and in 5% of chromosomically normal foetuses.
Combined screening: This test consists in the combined use of the PAPP-A and free B-hCG markers (the most frequently used markers, although others can be added to the test) and echographic markers (the most common is nuchal translucency, although others can be added). This screening method achieves the best results in the first trimester.Second trimestre
Biochemestry screening: In this test, maternal blood is analysed between the 14rh and 20th week of gestation to determine the presence of certain biochemical markers. Depending on the marker used, the test will be referred as:
Double test: (alpha fetal protein) and B-hCG Triple test: AFP , B-hCG and uE3 (non-conjugated estriol) Quadruple test: AFP , B-hCG, uE3 and Inhibine-A At present it is standard procedure to assess two or three markers, although new markers are currently being studied that promise to be of great future utility.
Echographic screening: The different echographic markers described for the second trimester are used between the 18th and 22nd week of pregnancy, coinciding with the second morphological ultrasound (an ultrasound that studies foetal anatomy). Echographic markers differ greatly from one another and their significance for risk of chromosomal alteration is different for each of these markers. The most frequently used echographic markers include:
Nuchal fold assessment, which consists in the measurement of the thickness of the foetal neck between 18 and 22 weeks. Generally, a nuchal fold below 6 mm between the mentioned 18 and 22 weeks is normal in most cases; however, when the nuchal measures over 6 mm, it is indicative of increased risk of Down syndrome.
Cysts in the choroid plexuses may be present in different number and size along the thickness of choroid plexuses, which are structures located in the cerebral ventricles. Their presence increases the risk for trisomy 18, although they are present in about 2% of normal foetuses and disappear totally between the 25th and 28th week of pregnancy. At present there is wide consensus on the advantages of combining the information provided by echographic and biochemical markers.Sequential screening
This modality of screening modifies risk as the results of new explorations become available. For instance, in a childbearing woman who had a combined screening in the first trimester with a risk of 1:1000, the presence of echographic markers for chromosomopathology in the morphological ultrasound will increase the risk in 1:200 or more, whereas the absence of echographic markers in the ultrasound will decrease the risk to 1:5000 or less.
Let’s see:
Integrated screening: This test takes into consideration the PAPP-A and Beta-hCG values obtained during the first trimester of pregnancy and the values obtained during the second trimester.
To increase the reliability of this test, other results are considered as the ultrasound results of the nuchal translucency, performed during the first trimester of pregnancy, and the nuchal fold results performed during the second trimester of pregnancy.
Other ultrasound markers, called “soft markers” such as the length of the femur, humerus, hypoplasia of the mild phalange of the small digit, absence or hypoplasia of nasal bone, measurement of iliac bone, dilated renal pelvis, cardiac defects, etc.
The combination of the results obtained through the biochemical screening and the ultrasound examinations allows the clinician to recalculate the risks depending on the maternal age, race, weight , absence or presence of insulin-dependent diabetes, number of children (twins, triplets). The pregnancy will be considered to be at risk when the risks exceed a certain threshold (or cut-off point), which is generally estimated at 1 in 250. Sensitivity is high, standing at about 90%, with a 3% rate of false positive, the results are not reported until all the tests have been done, which is approximately during the 16th week of pregnancy.
In cases where the expecting mother starts a late consultation in the office and it is not possible to perform the ultrasound examinations or biochemical screening tests of the first trimester, it is possible to still diagnose abnormalities in about 85-90% of cases by combining the ultrasound markers of the first trimester + the biochemical screening tests of the second trimester.
Screening of neural tube defects
Biochemical screening
This test determines AFP values in maternal blood. This blood test must be performed in the second trimester between 15 and 18 weeks and not before the 15th or after the 20th week. There is risk for the existence of neural tube defects if AFP values are over 2-5 MoM. AFP levels can also be determined in the amniotic fluid. Risk exists when the amniotic fluid is above 2 MoM. Some situations such as vaginal bleeding can also increase AFP values, a situation which invalidates it as a screening method.
Echographic screening
This screening method is used to visualise the integrity of the vertebral column and the normality of intracranial structures in the morphological ultrasound. Currently some centres that perform combined screening tests in the first trimester and are equipped with a high-resolution ultrasonography do not deem necessary to screen neural defects by biochemical screening, because they considered echographic screening to be sufficient.
In summary: AFP values are used to detect possible defects of the neural tube, such as open spina bifida and anencephalia.
Whenever increased values of alpha-fetoprotein are detected, an ultrasound examination should be performed to determine the exact gestational age, a diagnosis of multiple pregnancy or to detect fetal-placental structural defects. According to the results, amniocentesis may be required.
If AFP levels in maternal blood are higher than 2.5 MoM or higher than 2 MoM in amniotic fluid , it is possible to measure acetylcholinesterase levels in amniotic liquid as a diagnostic test to screen for neural tube defects. Please remember, the attainment of a pathological result when maternal screening tests are done is only an indication ON THE POSSIBILITY of some abnormality, but it DOES NOT confirm its existence.
Screening for cardiopathies
Measurement of nuchal translucency thickness (measurement of the fetal neck thickness) is also a good marker of cardiopathy. In foetuses that present a nuchal translucency above 3mm and a normal kariotype (obtained by invasive means), it is advisable to perform a foetal echocardiography to rule out the presence of a cardiac malformation. The presence of an abnormal flow wave pattern from the ductus venous also increases the risk of cardiac malformation.
Screening in multiple pregnancies
In twin pregnancies it is possible to use either the biochemical screening or the echographic screening, whereas in pregnancies of more than 2 foetuses only the echographic screening is normally used.
Most computer programs are designed to calculate the risk in twin pregnancies. The use of biochemical markers on their own determines the risk of the pregnancy itself (not the risk for each foetus), whereas echographic markers, or the combination of both, assess the specific risk for each foetus.
In summary: the fiability of the biochemical test using the mother’s blood it is lower because all fetuses contribute towards the final concentration of the substances measured using the mother´s blood, which could lead us to wrong interpretations.
- Can biochemical screening and free-fetal DNA screening be performed at the same time?
It makes no sense if any of the two has been performed and the results have been normal.
If in the absence of ultrasound abnormalities, the first test, that is biochemical screening, is performed and it is positive, before performing an invasive test that involves some risk of miscarriage, the free-fetal DNA screening test should be performed and if this test is also positive for some pathology, then it is recommended that an invasive test (chorionic villus sampling, amniocentesis, cordocentesis) be performed to rule out these or other chromosomal abnormalities not detected by this type of test.
If both tests (biochemical and free-fetal DNA) have been normal, but on ultrasound fetal malformations are observed, an invasive test (chorionic villus sampling, amniocentesis, cordocentesis) should be performed to rule out other chromosomal abnormalities that are not related to chromosomes that were studied in the screening.
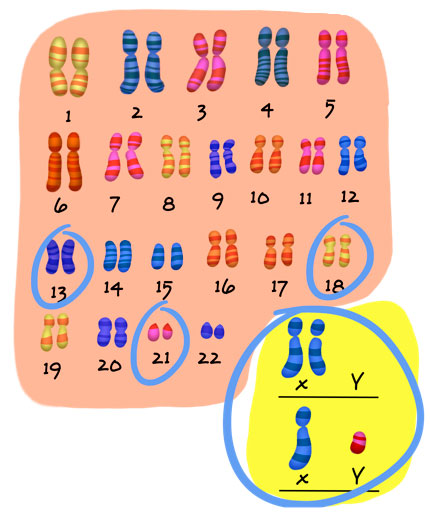
Remember that the human species has 23 pairs of chromosomes and that the chromosomes that are routinely studied with these techniques are: 13, 18, 21, optionally the X, Y chromosomes, and in some cases, microdeletions of some of them.
- What is nuchal translucency?
Nuchal translucency or nuchal oedema is an ultrasound marker of the first trimester (8-14 weeks of pregnancy), that consists in the measurement of the physiologic liquid accumulated in the baby’s neck via ultrasound.
Nuchal translucency increases physiologically with the gestational age, and can range between 2.4 mm at 12 weeks of pregnancy, to 2.9 mm at 14 weeks.
At present, the measurement of nuchal translucency has become the most sensitive and easy to obtain marker for the detection of some fetal pathologies, being present virtually in all foetuses between weeks 8 and 14 of pregnancy.
The space is measured from the external surface of the cervical column to the internal part of the cutaneous area, appearing upon ultrasound as a well circumscribed echonegative area.
If you require specific information on the position the foetus must be in at the time of the measurement, this link can be of help.
What is the best time to perform this test?
The nuchal translucency test can be performed from the 8th to the 14th week of pregnancy. After the 8th week by jeans of 3D vaginal ultrasound (three dimensional), but the ideal time to detect any abnormalities is between week 11 and week 13+6 days of pregnancy by jeans of 2D (bi-dimensional) vaginal or abdominal ultrasound, or 3D.
As a general rule, nuchal translucency is a transitory marker that disappears after the 14th week.
However, be careful with this information! Abnormal results can persist physiologically in about 2% to 4% of normal foetuses due to delayed closure of the upper part of the vertebral column or may also be pathological in cases of chromosomal abnormalities, malformative syndromes or other conditions that are not related to chromosomal abnormalities.
When is nuchal translucency considered normal?
Nuchal translucency is considered physiological when:
- Its thickness is less than 3 mm
- It is homogenous and lineal
- It is homogenous and lineal
When is nuchal translucency considered pathological?
It is suspected to be pathological when:
- Its thickness if over 3 mm.
- It is not lineal and small septa or irregularities are observed.
- The translucent space has a variable refringence.
- The atlas and axis (bones of the upper part of the vertebral column) remain open after the 12 week of pregnancy.
- When bullae or cystic structures are observed.
- Translucency extends beyond the cephalic pole or fetal back.
- When it is accompanied by ascitis or fetal anarsarca
- When other accompanying abnormalities are detected.No es lineal y se observan pequeños septos e irregularidades
For further information:
Book: Ultrasonidos 3D-4D en Obstetricia.
Authors: F. Bonilla-Musoles, L.E. Machado
Medical Publishers, panamericana, 2005.What can be done when the nuchal translucency test is positive?
The most important thing is NOT to get alarmed and to follow your doctor´s orders. When nuchal translucency is assessed, your doctor will take into account other biochemical studies performed during the first trimester and will subsequently give you guidelines that you will have to follow, among these:
- Ultrasound follow up of the foetus
- A study of fetal chromosomes by jeans of a chorionic biopsy or amniocentesis
How should we evaluate a positive nuchal translucency?
The risks for chromosomal abnormalities are calculated taking into account the ultrasound findings and the biochemical screening results obtained from the maternal blood.
For a nuchal translucency of 4 mm, the risk of chromosomal abnormalities is approximatelly 20%; for a nuchal translucency of 5 mm, the risk is 33%; for a nuchal translucency of 6 mm, the risk is 50%, and for a nuchal translucency greater than or equal to 6,5 mm, the risk is 65%.
PThus, the first step in the management of these pregnancies is to perform a fetal chromosomal assessment via a chorion biopsy.
For further information, log onto The Fetal Medicine Foundation.
Nevertheless, let’s NOT forget that certain abnormalities observed during the first trimester can correspond, in some cases, SIMPLY to transitory physiological or pathological situations that disappear leaving no evident sequelae in the newborns,
BECAUSE OF THIS, REMEMBER THAT AN ABNORMAL NUCHAL TRANSLUCENCY RESULTS IS ONLY INDICATING THE POSSIBILITY OF A GREATER RISK FOR SOME DEFECT and that subsequent studies will confirm or rule out such hypothesis.
Why is it necessary to continue having ultrasound examinations after a positive nuchal translucency and a normal chromosomal study?
- Because although most foetuses that present with increased nuchal translucency and a normal karyotype will be normal babies, it is advisable to exclude in these cases abnormalities such as cardiac defects, diaphragmatic hernia, skeletal dysplasias, renal defects, obstructive renal disease, onphalocele, as well as some other rare genetic syndromes (Noonan, Smith-Lemli-Opitz, Stickler Artrogriposis or multiple pterigium syndrome, etc.).
- PBecause 30% of translucencies greater than 5 mm are associated with disorders linked to higher perinatal morbimortality that are not related with chromosomal abnormalities. The aim of these ultrasound examinations is to assess the foetal wellness.
For that reason, in cases of increased nuchal translucency > 3mm and normal foetal karyotype, a detailed scan, including a foetal echocardiography (a study of the heart) should be performed between the 14th and 16th week of pregnancy to ascertain the progression of the nuchal translucency and to exclude or diagnose multiple foetal abnormalities. A detailed ultrasound examination should also be performed at 20-22 weeks to either exclude or diagnose more subtle malformations or defects associated with genetic abnormalities. If everything is in order, the risk to give birth to a newborn with a severe abnormality or psychomotor retardation is not higher than that of the general population.
What is the nuchal skin fold?
This is an ultrasound marker used in the second trimester of pregnancy consisting in the measurement of the thickness of the subcutaneous tissue at the level of the baby’s neck. This test should be performed between the 14th and 22nd weeks of pregnancy and it is considered pathological when it is above 6 mm.
In foetuses with Down’s syndrome (trisomy 21), this value is increased.
Please note, do not confuse “nuchal translucency” with “nuchal fold”, as these are two different ultrasound markers.
For further information:
The Fetal Medicine Foundation.
Book: Ultrasonidos 3D-4D en Obstetricia.
Authors: F. Bonilla-Musoles, L.E. Machado
Medical Publishers, panamericana, 2005.
Next topic: Where are we now and where are we headed
Reviewed: 19th of January 2015