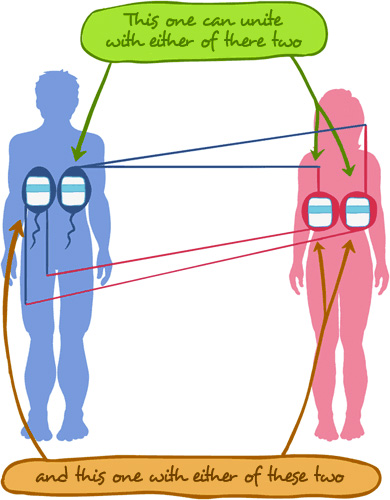
What happens when our recipes combine with our partner’s recipes?

Well, each member of the couple, irrespectively of what their personal combination might be, will find that the other partner may express any of the previously mentioned combinations for any given recipe. Based on these recipes, at the time of fertilisation, the different combinations, giving the different probabilities of presenting some trait or hereditary disorder, will be appear.

Let’s get to the point and see what happens in practice.
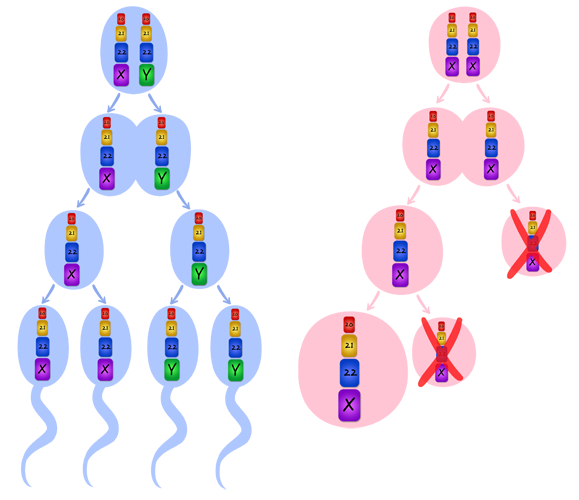
As stated previously, in order for the number of chromosomes to remain constant and for germinal cells to be able to fertilise, a reductional division or meiosis has to occur. To explain the risk percentages in the different types of heredity, we will focus on the type of cells that are produced immediately after reductional division has taken place, as these are the only possible resulting combinations.
Under normal conditions in a woman, one of these cells is lost. Since we do not know which one of them will be lost, and one cell complements the other, both will be studied. These are the only two possible combinations and any of the two can occur.
From now on we will only refer to one single character encoded by the same chromosomal set, which will be represented as follows:
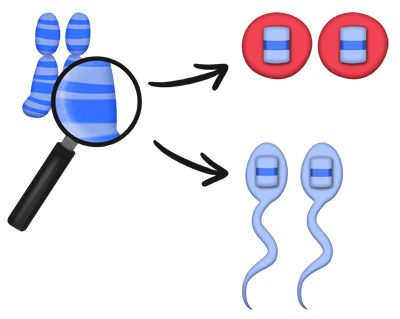
Given that each of us has two chromosomes from each set, our resulting gametes will be these.
And our partner’s gamete will be these.
We will always be talking about the same recipe within the same chromosomal set, for both members of the couple.
And now let me give you a graphic representation of the different combinations that can result in reproduction.
If we pay close attention we will see that we are all a mixture of all the characters that run in our family. Our hair can be the same colour as that of our maternal grandfather and our eyes can be the same colour as our paternal grandfather’s, the hands may resemble our maternal grandmother’s and the teeth can be exactly like our father’s.
For sure, you will ask yourselves: How is this mixture possible?
Well, it is extremely easy. Chromosomes of a same set exchange information between them before they undergo reductional division or meiosis. That is, recipe number 4 from chromosome number 1 is exchanged for recipe number 4 from the other chromosome number 1, and this same process is repeated in many other recipes.
In the end, the resulting chromosomes are a mixture of all the recipes or characters from our ancestors.
And it is thanks to this exchange that the variability of the species prevails, making each of us different from the other, unique and unrepeatable.
But, for every thing to come out right, each chromosome of the same set must contain the same recipes at the end of this process, irrespectively of whether they have been exchanged or not, so that each chromosome has all the recipes it needs, without a single one missing or in excess.
And, which different combinations can result when we reproduce?
You have different options:
- Read through all the combinations, which will provide you with a global view. We recommend this option as it will enhance your overall understanding as to how we fight disorders today.
- Read through only a few pages starting at the beginning, so that you become familiar with how these combinations give rise to disorders.
- And if you are at specific risk, because you fall into any of the situations described, I suggest that you first read everything and then come back to the section that concerns your particular case.
As you can see, it is very easy.
Autosomal disorders
 Let’s imagine any set of chromosomes inside the first 22 sets, and one of these 22 sets of chromosomes contains the wrong or PATHOLOGICAL recipe that we will identify as “P” , and a second recipe with the correct information that we will identify as “c” .
Let’s imagine any set of chromosomes inside the first 22 sets, and one of these 22 sets of chromosomes contains the wrong or PATHOLOGICAL recipe that we will identify as “P” , and a second recipe with the correct information that we will identify as “c” .
This system of symbols will be applied to autosomal dominant disorders as well as to autosomal recessive disorders.
In all the situations that will be described next, it is assumed that we will ALWAYS be referring to the same recipe or character within the same particular chromosomal set, but always to the same set in both members of the couple.
For instance, let’s assume that we are referring to a recipe or character located in chromosome number 6; what is represented graphically is the same recipe in both chromosomes number 6 for each member of the couple, that is to say, the male’s chromosome and the female’s chromosome. This is a very important detail! DON’T EVER FORGET!
This group of disorders includes the following progenitor situations or combinations:
Autosomal dominant
Please, remember that the pathological nature of this type of heredity, as it is DOMINANT, is always expressed.
- Affected individual who has one Pathological recipe and one correct recipe and reproduces with a healthy individual
Affected individual

 who has one Pathological recipe and one correct recipe and reproduces with a healthy individual
who has one Pathological recipe and one correct recipe and reproduces with a healthy individual 
An individual, with an autosomal dominant disorder, is going to produce after meiosis a gamete with the chromosome that contains the correct information and a second gamete with the chromosome that contains the Pathological or different information.
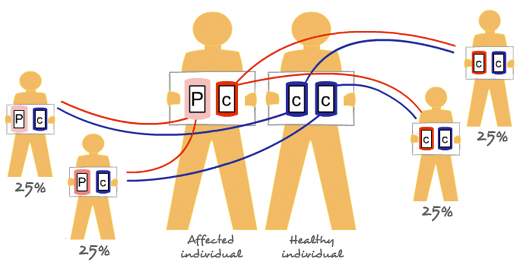
When reproducing, the normal thing is for the said individual to mate with another individual who has the correct information in both chromosomes. In this case, the risk of the couple to borne offspring that is affected is 50%, regardless of whether the kids are boys or girls (please remember that we are referring to the first 22 sets of chromosomes and these are the same in men and women, and thus the gender of the particular individual has nothing to do with the process).
In other words, 50% will be
: Healthy individuals, as both their recipes are correct.
And the remaining 50% will be : Affected individuals, as they have a good recipe and a Pathological or altered recipe. - Affected individual that reproduces with another affected individual for the same anomaly, that is, they both have the same disorder
Affected individual
that reproduces with another affected individual  for the same anomaly.
for the same anomaly.That is, they both have the same disorder.
In this case, the expected offspring will be as follows:
75% of the offspring will be affected. Of these, 50% will have a normal gene and an abnormal gene. That is they will be heterozygotes:
- 25% + 25%
- And the remaining 25% will carry both Pathological or anomalous genes , that is they will be homozygotes.
Probably in this 25%, the disorder will most likely manifest itself in a much more severe form.
The other 25% of the offspring will be healthy
because the two chromosomes they inherit contain the correct information. Because these children do not have the disorder and their genes or recipes contain the correct information, they will not pass on the disorder to their descendants. - 25%
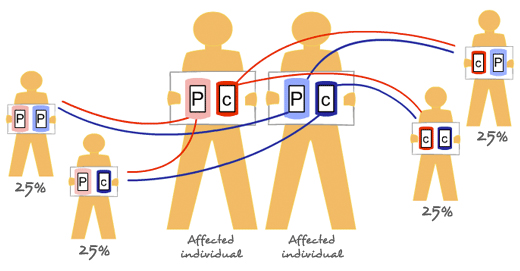
- Affected individual with two Pathological or incorrect recipes who reproduces with another affected individual who also has two Pathological incorrect recipes
Affected individual with two Pathological or incorrect recipes
who reproduces with another affected individual who also has two Pathological incorrect recipes 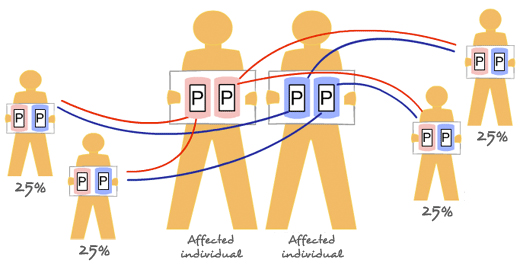
In this case, all their offspring will be affected and, moreover, both recipes will be Pathological or incorrect in all the children
- Affected individual with two Pathological or incorrect recipes who reproduces with another affected individual who has one correct and one Pathological or incorrect recipe
Affected individual with two Pathological or incorrect recipes
who reproduces with another affected individual who has one correct and one Pathological or incorrect recipe 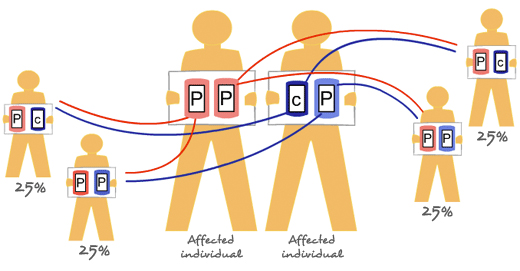
In this case, all offspring will be affected.
- Of the affected offspring, a 50% will have an incorrect recipe and a correct recipe,
- and in the remaining 50% both recipes will be incorrect
- Of the affected offspring, a 50% will have an incorrect recipe and a correct recipe,
- Reproduction between an individual who carries two Pathological or incorrect recipes and another individual who carries two correct recipes
Reproduction between an individual who carries two Pathological or incorrect recipes
and another individual who carries two correct recipes 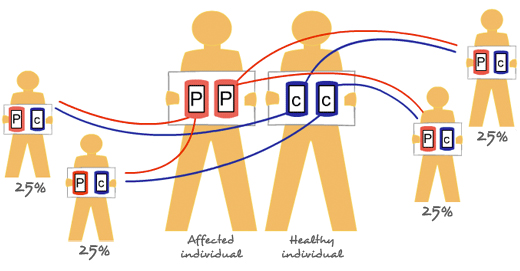
All the children will be affected and they will all be carriers of an incorrect recipe and a correct recipe
Autosomal recessive
Because these are autosomal disorders, we will now continue to analyse the first 22 sets of chromosomes.
Let´s not forget that the pathological character in this type of inheritance remains in recess or hiding if it is accompanied by the healthy dominant character.
- A healthy non-carrier individual who reproduces with a healthy carrier individual
A healthy non-carrier individual
who reproduces with a healthy carrier individual 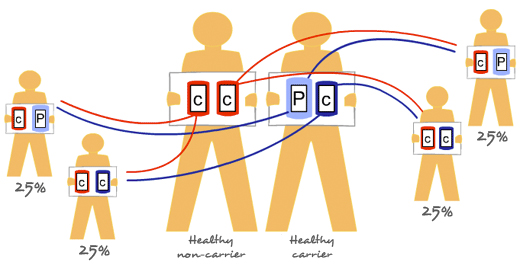
The type of expected offspring will be distributed as follows:
- 50% of healthy carriers
- 50% of healthy non-carriers
In this case, as you can see, all the resulting offspring will be healthy, and of these children, 50% will be asymptomatic carriers
. In other words, they will not present any symptom or any manifestation of the disorder.Since we all carry some incorrect recipes, we are all on the same boat. It is only when we reproduce with an individual who has the same incorrect recipe like ours that we will run a 25% risk of having children afflicted with autosomal recessive disorders. We will then be in the following scenario: (Option B).
- 50% of healthy carriers
- Healthy non-carrier, individual who reproduces with an affected individual, that is, someone with two Pathological or incorrect recipes
Healthy non-carrier, individual
who reproduces with an affected individual , that is, someone with two Pathological or incorrect recipes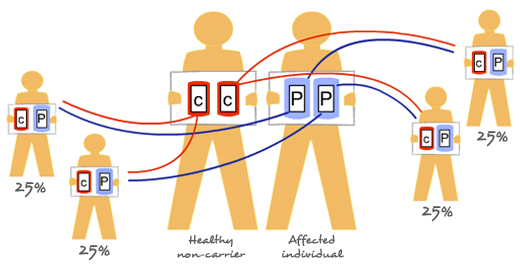
As you can see, all the children resulting from this combination will be healthy but carriers, since a recipe of each type have been passed on
- A healthy carrier who reproduces with another healthy carrier with the same pathologic gene
A healthy carrier
who reproduces with another healthy carrier with the same pathologic gene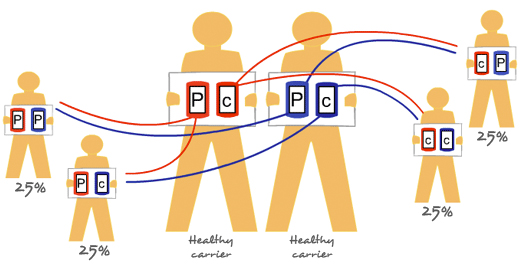
The expected offspring will be:
- 75% healthy offspring of which
50% will be healthy carriers because they have one correct recipe and one Pathological or incorrect recipe ( 25%
+ 25% )and the remaining 25% will be healthy non- carriers
, since both recipes are correct.- And, a 25% of affected children, because they will have inherited the two chromosomes with the incorrect recipe
Please remember that in autosomal recessive disorders, it is necessary to have both chromosomes with the two incorrect recipes (alleles) for the disorder to manifest. This is because if we have a good copy and a bad copy, the bad copy will not be expressed as it is in recess or hidden, and gene expression depends on the dominant recipe or allele.
This type of heredity is easily suspected when healthy parents produce several children who are affected with the same disorder, irrespectively of whether they are males or females, and mainly in small-sized population groups that only reproduce among themselves, populations with a very high rate of defective recipe or allele, and mostly when there is a past history of consanguinity. This is why marriage between members of the same family, for instance “blood cousins” is not advisable, as merely because they belong to the same family, the probability to have the same incorrect recipes is higher. On the other hand, if we reproduce with individuals from a different family, the probability of having the same incorrect recipes is clearly lower. Despite the fact that we all have incorrect recipes, these are not likely to be the same ones, and consequently, there is less probability of having children affected with autosomal recessive disorders.
For this reason, formerly, when a blood-related couple was going to have a religious wedding, the Church assessed the existing degree of kinship, and if the percentage of genes was too high, it denied them permission to get married. This process was known as consanguinity- related dispensations.
- Affected individual that reproduces with another affected individual
Affected individual
that reproduces with another affected individual Let’s keep in mind that we are always referring to the same pathology.
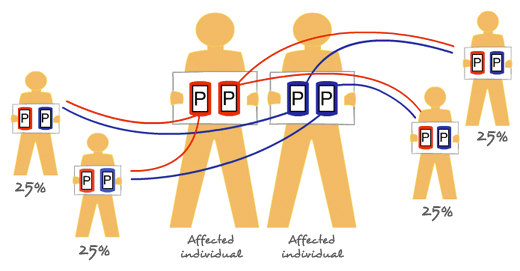
In this case, all offspring will be affected because both inherited recipes are incorrect
- Affected individual who reproduces with a healthy carrier of same pathology
Affected individual
who reproduces with a healthy carrier of same pathology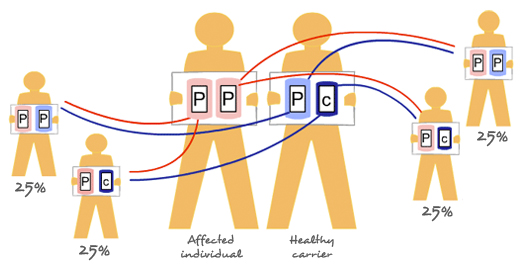
In this couple the probabilities are:
- 50% affected children, as their combination is
- and 50% of healthy children who are carriers because of their combination
- 50% affected children, as their combination is
Sex linked disorders (X-chromosomes disorders)
 Please remember that, as indicated by their name, this type of disorders are related to or influenced by the carrier’s gender.
Please remember that, as indicated by their name, this type of disorders are related to or influenced by the carrier’s gender.In this group, there can be two possible scenarios: that the pathological “X”-chromosome is carried by the female or the male, and that, in turn, this X-chromosome-linked character is expressed in a dominant or recessive way.
To identify the “X” -chromosomes that are contained in the incorrect recipe, this symbol will be used: 
Please do not forget that we are always referring to the same character or allele located in the X -chromosome, both in the man and in the woman alike.
“That is, we are always referring to the same recipe in both genders”.
X-linked dominant disorders
PLEASE REMEMBER that in this case, the X chromosome with the wrong recipe, in the presence of another X chromosome with the right recipe, will express because it is dominant, IN OTHER WORDS, IT DOMINATES THE SITUATION.
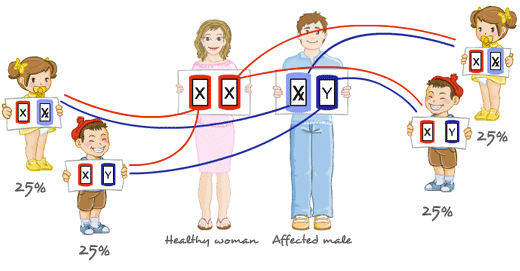
- Healthy woman who reproduces with an affected male
Healthy woman
 who reproduces with an affected male
who reproduces with an affected male 

 View animation
View animation The expected offspring will be as follows:
- 50% affected women
- 50% healthy men
In this case, all the male children will be healthy because they inherit the father’s Y – chromosome, while all the daughters will be affected because they receive the father’s X- chromosome, which in this case is pathological.
The fact that all the daughters of an affected male are affected and all the sons are healthy, allows us too distinguish between a family with an autosomal dominant disorder and another with a X-linked dominant disorder. In dominant autosomal disorders, the affected male transmits the pathological gene to both males and females, as it is not gender-dependent.
- 50% affected women
- Affected woman that reproduces with a healthy male
Affected woman
 that reproduces with a healthy male
that reproduces with a healthy male 
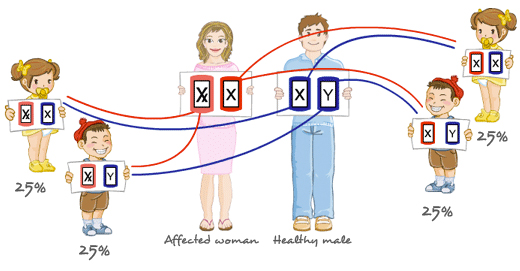
The expected type of offspring will be:
- 25% of healthy females
- 25% healthy males
- 25% affected females
- 25% affected males
In synthesis, if we focus on males only, we can see that each male has a 50% chance of being healthy and a 50% chance of being affected. And the same thing happens if we focus on women only, each woman has a 50% chance of being healthy and a 50% chance of being affected.
REMEMBER that dominant characters, even if they are present in one single dose, are always expressed. Thus, in this particular case, and despite the fact that we are looking at sex chromosomes, if a woman has a X chromosome with the incorrect ” X ” recipe, and the other chromosome contains the correct recipe, she will express the disorder, given that the same concept as for autosomal dominant disorders applies because two X chromosomes are shared and one of them is incorrect.
As regards the male, it will depend on which of the two X chromosomes he has inherited, the “good one” or the “bad” one.
- 25% of healthy females
- Affected woman with one pathological recipe who reproduces with an affected male
Affected woman with one pathological recipe
who reproduces with an affected male 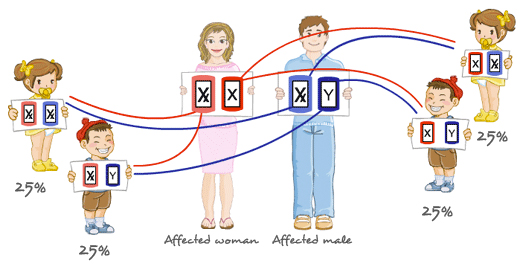
The expected type of offspring will be:
- 50% affected women of whom:
25% have one correct recipe and one incorrect recipe
25% in whom both recipes are incorrect- 25% of healthy males
- 25% of affected males
That is, if we take males only, we can see that each male has a 50% chance of being healthy and a 50% chance of being affected, whereas if we take women only, they will always be affected because they inherited their father’s X-chromosome (and in this case, it is pathological).
- Affected woman with two pathological recipes who reproduces with an affected male
Affected woman with two pathological recipes
who reproduces with an affected male 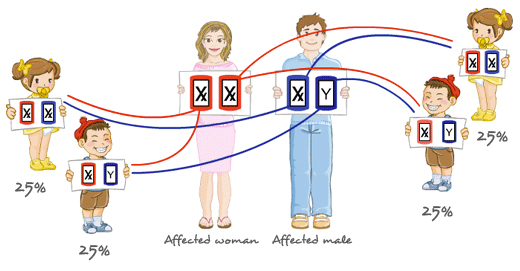
In this case, the entire offspring will be affected:
- the males because they inherit a pathological chromosome from the mother,
- and the females because they inherit a pathological chromosome from the mother and also the pathological chromosome from the father, so both recipes will be incorrect.
- the males because they inherit a pathological chromosome
- Affected woman with two pathological recipes who reproduces with a healthy male
Affected woman with two pathological recipes
who reproduces with a healthy male 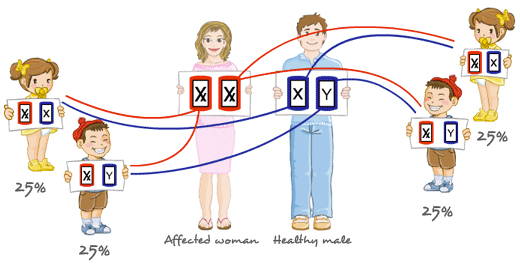
In this case, all the offspring will be affected and the females will have a correct and an incorrect recipe.
X-linked recessive disorders
Remember that in this case, the X chromosome with the wrong recipe , in the presence of another X chromosome with the normal recipe, will not express itself because it is in recess or hidden.
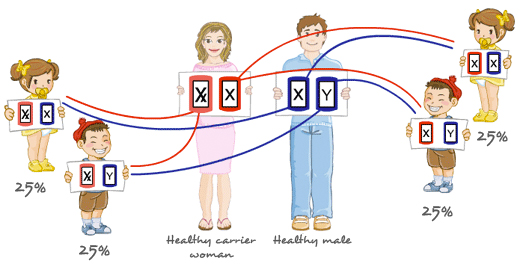
- Healthy female carrier who reproduces with a healthy male
Healthy female carrier
who reproduces with a healthy male If the female is the carrier, she does not express the disorder, but during meiosis or reductional division, two types of gametes will be produced, one that has a normal X chromosome and one that has a mutated X chromosome, therefore, according to the sex that this child has after the paternal contribution, the probabilities are as follows.
Offspring will be as follows:
- 50% all healthy females, of which:
25% are healthy non carriers
25% are healthy but carriers- 25% healthy males
- 25% affected males
Therefore, if we just focus on males only, each male has a 50% probability of being healthy and a 50% probability of being affected. Whereas if we focus on females only, they will always be healthy, although a 50% of them will be carriers.
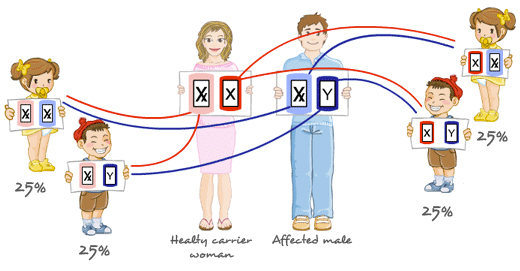
- Female healthy carrier who reproduces with an affected male
Female healthy carrier
who reproduces with an affected male The expected type of offspring will be:
- 25% healthy females but carriers
- 25% affected females because both recipes are wrong
- 25% healthy males
- 25% affected males
Therefore, each male has a 50% probability of being healthy and 50% probability of being affected, whereas each female has a 50% probability of being healthy but a carrier and a 50% probability of being affected.
- 25% healthy females but carriers
- Healthy non carrier female who reproduces with an affected male
Healthy non carrier female
who reproduces with an affected male 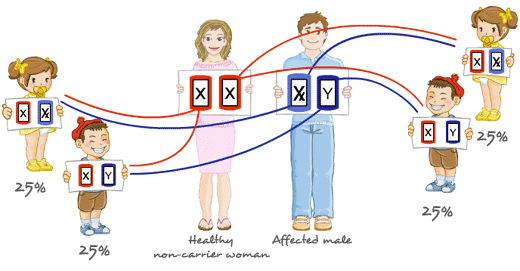
The type of expected offspring will be:
- 50% healthy females but carriers
- 50% healthy males
In this case all their children will be healthy because:
the males inherit the Y chromosome from their father,
the females will all be healthy, but all of them carriers, because although they inherit the X chromosome from their father which is pathological, it is compensated by the X chromosome they inherit from their mother, which is normal. - 50% healthy females but carriers
- Affected woman who reproduces with an affected male
Affected woman
who reproduces with an affected male 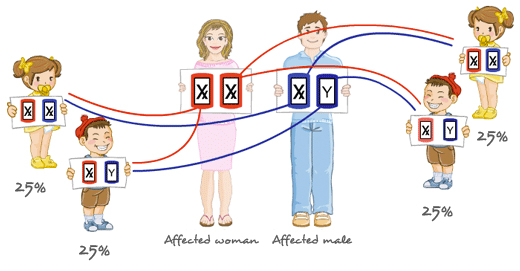
In this case, the entire offspring will be affected.
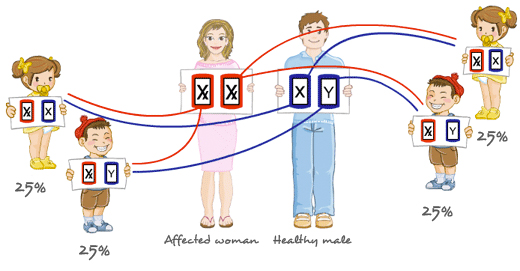
Please note that the females are affected because both their recipes are defective. - Affected woman who reproduces with a healthy male
Affected woman
who reproduces with a healthy male The expected offspring will be:
- All healthy females but carriers.
- All affected males.
Having seen how hereditary diseases are transmited, if you require specific information on a certain disease, the following links can help you.
And please, regardless of all the information you get on the subject of your interest, do not forget that it is only an information service, containing data that must be interpreted by a specialist, so please before you make any decision, have a consultation with a Genetics department, where your individual case will be accurately assessed and where all your questions will be answered.
Where does all this take us?
Well, it is easy, when one of the progenitors is sick, or one or both of them are carriers of the same genetic disorder, they have a risk to produce affected children. The amount of risk and the sex of the affected individual is dependent on the type of inheritance.
For this reason, in case a malformation or a family disorder exists, the first thing to do is to study the family background and see which inheritance pattern runs in the family.

To this end, a genealogical tree is made using an international nomenclature in which all the individuals appear, identifying those who are affected and once these are identified, to determine the degree of severity, because we know that, in some cases, this can vary among the particular individuals.
¡Remember that the final flavour depends on all the ingredients mixed in the pie!
In case that the disorder or malformation is not diagnosed, appropriate exams must be performed to try and obtain a diagnosis, and on the basis of this diagnosis, the risk of the particular individual to produce children with the same problem is calculated.
Some of these disorders are very severe, so at the time of deciding on their reproductive future, couple may encounter the following situations:
- They ACCEPT the prenatal diagnosis, if available for this particular disorder, regardless of whether they decide to terminate or go ahead with the pregnancy.
- They DO NOT ACCEPT the prenatal diagnosis.
Related questions
- Why are blood-related individuals more likely to have the same mutations causing the disease?
Because both SHARE THE SAME COMMON ANCESTOR, and if this ancestor had pathological genes, these could have been transmitted from generation to generation.
Because we know that the PROBABILITY of having inherited the same gene is directly proportional to the degree of kinship; in other words, the closer the kinship relationship, the greater the chance of having inherited the gene.
To take an example: let’s go check out the third option of autosomal recessive diseases described above, because it is the most common situation among relatives, reproduction between two healthy individuals who are both carriers of the same pathological hidden recessive gene.
“Healthy individual
who is a carrier that reproduces with another healthy individual who also happens to be a carrier “.We can see that merely because that both progenitors share the same ancestor they have much higher chances, compared to the general population, of both being carrier of the same pathological gene or genes. And this significantly increases the probabilities (by a 25%) that when reproducing, the offspring may inherit the affected gene and manifest the disease because he or she has inherited the same wrong recipe from each of the two progenitors. That is, a baby with both affected genes or wrong recipes (homozygous) for a particular gene.
In contrast, if reproduction takes place with an individual that does not belong to the same blood- related family, these possibilities go down to the risk of the general population; that is, the risk continuous to exist but it is much lower.
And, do you know why there is still a small risk?
Because it has been estimated that each person carries between one and five recessive lethal mutations that would be lethal if the children inherited them in the homozygous state. Therefore, all mankind carries pathological genes. We also know that there are pathological genes that are much more common in certain groups or human populations. Hence, if we belong to any of these population groups, we run a much higher risk to reproduce with a healthy carrier like us, which even if there is no family blood connection, will lead to a higher chance of having a child that has inherited the mutations.
- How is the degree of kinship measured?
The table below on consanguineous crossings explains how.

Please note that in this case, it is of outmost importance to take into account:
1) Degree of kinship
You can consult the definition of degree of kinship on the Wikipedia.
2) Endogamy coefficient for the offspring
It is the probability for the offspring (new individual) to have inherited from the progenitors the same genes or recipes from the same-shared ancestor for a percentage of such individual´s genome.
Type 1
↓
Kinship degreeProportion of shared genes 2
↓
Child´s endogamy coefficientIdentical twins
(view in Wikipedia)– 1 = 100% – Progenitor-child 1º 1/2 = 50% 1/4 = 25% Brother-sister (including dizygotic twins / non-identical)
(view in Wikipedia)1º 1/2 = 50% 1/4 = 25% Brother-half sister 2º 1/4 = 25% 1/8 = 12,50% Uncle-niece or aunt-nephew 2º 1/4 = 25% 1/8 = 12,50% Half uncle-niece 3º 1/8 = 12,50% 1/16 = 6,25% Blood cousins 3º 1/8 = 12,50% 1/16 = 6,25% Double first cousins 2º 1/4 = 25% 1/8 = 12,50% Half cousins 4º 1/16 = 6,25% 1/32 = 3,13% Second cousin 4º 1/16 = 6,25% 1/32 = 3,13% Third cousins 5º 1/32 = 3,13% 1/64 = 1,61% OBSERVATIONS
- The absolute genetic risk of having anomalous offspring (spontaneous abortions, congenital malformations, neonatal deaths) for the descendants of any non-related couple is 2-3%.
- The absolute genetic risk of having anomalous offspring (spontaneous abortions, congenital malformations, neonatal deaths) for the descendants of cousins is 3-5% (nearly two-fold).
- The risk of having abnormal offspring is practically insignificant starting from third cousins or between more remote kinships.
- Consanguinity between parents and children and between siblings (incest) has a very high risk for malformations and mental retardation.
Next topic: Origin of hereditary disorders
Reviewed: 25th of September 2017