- Home
- Prenatal diagnosis
- Assisted Reproduction Techniques
Assisted Reproduction Techniques
We should keep in mind that gametes must first be produced, then they must find each other; and finally, if fecundation has occurred, they must be implanted in the uterus.
Now let’s see how we influence each stage.

Gamete production of formation stage
THIS PHASE CANNOT BE MANIPULATED, because presently it is not possible to manufacture gametes, chromosomes, or their genes.
But, we can do the following:
In case of a hereditary disorder, infer the expected proportion of affected gametes and determine the type of chromosomes they belong to (autosomes or sexual chromosomes);
And on the other hand, obtain or retrieve the gametes (be them ova or spermatozoa) to study them, or as we will see further on, make their encounter possible at our convenience.
So that, once they are formed, they can be collected and stored in the Laboratory under special conditions so they do not spoil.
¿How can this be done?
Remember that the female usually produces an ovum each month and the male in each ejaculation lets off millions of spermatozoa.
If a woman receives specific hormone treatment, instead of producing one ovum per month, she will produce many more. Ova can be subsequently retrieved and stored by means of an ovarian puncture under ultrasound guidance.
The collection process for the male is much easier because the semen is obtained through masturbation or during sexual intercourse using a spermicide-free condom. It is then deposited in a sterile recipient and saved under special conditions.
And once the gametes have been produced and saved, we enter the next phase.
Fertilization phase or gamete union

This is the ONLY phase that can be currently MANIPULATED or CHANGED.
Fertilization may occur inside or outside the female’s body.
For this purpose we employ a series of techniques known as ASSISTED REPRODUCTION TECHNIQUES, which allow us to modify or manipulate the union between the ovum and the sperm cell.
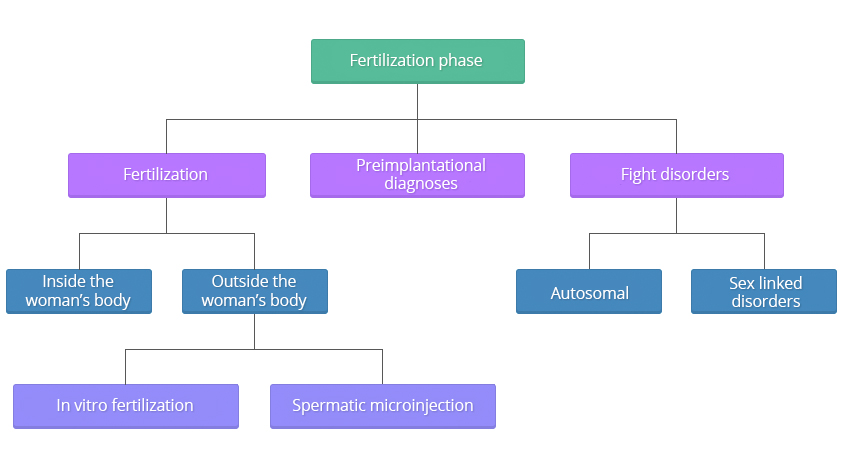
Fertilization
- Fertilization outside the woman's body
If fertilization occurs outside the woman’s body by means of assisted reproduction techniques, which are techniques that help the fertilization occur, we can use in vitro fertilization and spermatic microinjection.
In vitro fertilization technique
This technique consists in uniting the ova with the spermatozoa in a laboratory container so that the spermatozoa fertilize the ova.
Therefore the availability of the saved gametes and the ability to achieve fertilization outside the woman’s body provides us with many recombination possibilities between them, according to our needs and the specific problem involved.
In vitro fertilization can be achieved in:
- Couples who provide their own reproductive material, that is ova and spermatozoa.
- Donor material, either from a female origin: donation of ovocytes, or from a male origin : donor semen. In this case there can be different possible combinations:
- Ova from the woman with donor semen.
- Donor ova with semen from her partner.
- Donor ova with donor semen. In this case the reproductive material is not the couple’s genetic material.
Once the ovocytes have been fertilised and selected, depending on the prognosis of each case, the age of the woman, quality of the embryos, personal past history, etc. , a variable number of embryos is transferred into the uterus through the uterine neck. This number can vary between one and five, incompliance with the law in force in each country.
The remnant eggs are stored in a frozen state for future utilisation by the couple in a new cycle. This can be as a result of failure to get pregnant in the first attempt or simply because the couple may wish to have more children in the future. The success rate to achieve a pregnancy in each of these transfers is currently estimated to be at 40%.
The embryos can be stored for a variable length of time (from 5 to 10 years), during which time the couple may make use of their embryos at any time. If after this time, the couple decides not to use them, the future of the frozen embryos will depend on the legislation of each country.
This technique is used in cases where the Fallopian tubes are obstructed, in cases of infertility of an unknown origin, or in some hereditary diseases.
The transfer of more than one embryo can result in a multiple pregnancy.Spermatic microinjection
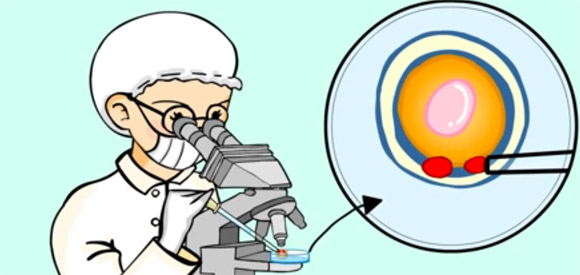
This technique helps the spermatozoon penetrate the ovum by eliminating as many obstacles as possible so that is able to fertilize. In simple terms, by piercing through the several layers that protect the ovum.
The technique consists in injecting a spermatozoon directly inside the ovum. This technique is known as ICSI (Intracytoplasmatic sperm injection of only one spermatozoon) and to date it has been able to resolve a number of male infertility cases where in vitro fertilization or other techniques of microinsemination have failed.

Preimplantational diagnoses
In turn, these assisted reproduction techniques enable us to perform PREIMPLANTATIONAL DIAGNOSES. In simple terms, they allow us to study and select those eggs or embryos that are health and have no diseases or pathology before they are transferred into the uterus.
This can be performed in two ways: PRECONCEPTIONAL and POSTCONCEPTIONAL.
- PRECONCEPTIONAL diagnoses
PRECONCEPTIONAL diagnoses
This means that the diagnostic procedure is performed on the gametes (ovum or sperm cell) in order to study and select only those which are healthy BEFORE they come into contact for subsequent fertilization.
In a WOMAN it is done through a biopsy of the FIRST polar corpuscle.
Polar corpuscles are “discarded” cells that are produced during the two cell divisions that the ovum undergoes during its maturation period.
The analysis of this cells will permit us to infer the genetic state of the ovocyte.
The first polar corpuscle is the first “discarded”cell that is produced during the first meiotic division.At the present time there is no effective method in MALES. However, we are looking into the following possibilities:
- To study spermatozoa through a technique called spermatic duplication.
- And, to separate spermatozoa that carry the “X” sex chromosome from spermatozoa that carry the “Y” sex chromosome. This will enable us to choose the right chromosome when sex-linked disorders exist.
- POSTCONCEPTIONAL diagnoses
POSTCONCEPTIONAL diagnoses
This means that the diagnostic procedure is carried out when fertilization HAS ALREADY taken place. In this case, the embryos are analysed before being transferred into the uterus. These technique enable us to select and transfer only those embryos that are free of disease or pathology.
This can be done as follows:
Biopsy of TWO polar corpuscles
This type of biopsy is used when the pathology to be ruled out only involves the woman, given that the two polar corpuscles originated from the ovum and the ovum is a female cell.
Biopsy of AN EMBRYONIC cell, day 3 of gestation
This type of biopsy allows the clinician to rule out pathologies of a male origin as well as pathologies from a female origin, as the embryo was formed from the building blocks of both parents.
Biopsy of FOUR or FIVE trophectoderm cells, precursor epithelium of the placenta, day 5 of gestation
English: 4 min 37 sec.In both cases (biopsy of embryoincs cells and biopsy of trophectoderm cells), a hole is performed using chemicals or laser dots in the zona pellucida of the embryo to obtain the embryonic material.
Once the embryo biopsies are performed, these are put under observation or frozen until the results come back and then they are transferred to the uterus.
When the origin of the pathology to be studied is of a female origin, the two polar corpuscles can also be removed at the same time together with the embryonic cell.
The more material we have to perform the study, the more certain and reliable the diagnosis will be.
Preimplantational diagnosis allows the clinician to perform a number of tests on:
- chromosomal alterations
- genetic alterations caused by an alteration or mutation of a specific gene (incorrectly or poorly written cool book recipes)
Among them:
Cystic fibrosis, Alpha and B-thalassaemia, Haemophilia, Sickle cell anaemia, Lesch-Nyham syndrome, Tay-Sachs disease, RhD blood typing, Medium chain acyl CoA dehydrogenase defficiency, Spinal muscular atrophy, Marfan´s syndrome, Myotonic dystrophy, Familial adenomatous polyposis coli, Retinitis pigmentosa, Huntington´s disease, Fragile X, Congenital adrenal hyperplasia, Duchenne muscular dystrophy, Charcot-MarieTooth (type 1A). Chromosome abnormalities

Before undergoing this type of study, each case must be assessed individually by the clinician, attending GP or specialised geneticist, in order to evaluated, the possibility to perform preimplantational genetic diagnosis.
It is advisable that all pregnancies resulting from preimplantational diagnosis be checked subsequently by means of prenatal diagnostic tests.
Spanish: 2 min 06 sec.
Fight disorders
Based on all these possibilities and the knowledge we have acquired on hereditary disorders, the risk and type of inheritance involved, and the availability of a prenatal or preimplantational diagnosis, and provided the couple accepts to undergo the test, the solutions currently available to fight the disorders are as follows:
- Sex linked chromosome disorders
Sex linked
 chromosome disorders
chromosome disordersAs in the previous cases, a prenatal diagnosis may not be available or if available, the couple may not agree to it.
We will first distinguish between dominant and recessive disorders. Once that differentiation is made, the gender of the progenitor who is a carrier or affected with the alteration will be taken into account for each disorder.-
Dominant
- If it is the woman who is carrying the pathological X chromosome, she will be affected, because in this case the gene is dominant and the following can be offered:
- Ovocyte donation.
- Specific preimplantational diagnosis, and if this does not exist, we cannot offer preimplantational diagnosis for embryo sex differentiation, because both sexes manifest the disease if they inherit the pathological X chromosome.
- If the pathological X chromosome is in the male, he will be affected. And we can offer the following:
- Donor semen insemination.
- Specific preimplantational diagnosis, and if it does not exist.
- Preimplatational diagnosis for embryo sex differentiation, transferring only the male embryos, because they are all healthy, as they inherit their father’s Y chromosome.
- If it is the woman who is carrying the pathological X chromosome, she will be affected, because in this case the gene is dominant and the following can be offered:
-
Recessive
- If the carrier is a female, we may offer the following:
- Ovocyte donation.
- Specific preimplantational diagnosis for the disease, and if this does not exist …
- Preimplantational diagnosis for embryo sex differentiation, this means to analyze and only transfer female embryos, because although some of the females will be carriers, at least they will be healthy. Instead with the male embryos, since at present one cannot distinguish who has inherited the pathological X chromosome and who has inherited the healthy X chromosome from the female, the best alternative is to eliminate them both to avoid transfer into the uterus.
- If it is the male who is carrying the pathological X chromosome, he is affected, but we must remember that all his offspring will be healthy, because the males inherit the Y chromosome from their father, and the females are also healthy because although they inherit the pathological X from the father, they also inherit the normal one from their mother, and since we are speaking of sex linked recessive inheritance, they are healthy carriers that do not express the disease. But when they reproduce, they have a 50% risk that their male children will be affected. Therefore, if we want to eliminate this last possibility, we can actually offer the couple the following:
- Donor semen insemination.
- Specific preimplantational diagnosis, and if this does not exist,
- Preimplantational diagnosis for male embryos sex differentiation because they all will be healthy since they inherit the Y chromosome from the father. And, in this case, we will avoid the transfer of female embryos since all of them will be carriers.
- If the carrier is a female, we may offer the following:
-
Implantation phase
Implantation or nesting CANNOT be manipulated.
However, nowadays there is the possibility to transfer the embryos into the uterus under ultrasound guidance aimed at depositing the embryos in the most suitable area inside.
Before the transfer, an anatomical and functional assessment of the uterus should be conducted to rule out any sort of pathological condition.
The administration of progesterone (via the vagina) can help the endometrium develop correctly (internal layer of the uterus where the embryo will be implanted). However, this can be performed only if the doctor deems it necessary.
Related questions
As you can see more and more solutions become available!
What must be clear is that, regardless of the technique used, the pregnancy in all these cases is carried by the woman of the couple. Only in some specific cases such as when the uterus of the woman does not exist or when it is not possible to use it due to the presence of prohibiting medical indications, a surrogate mother’s uterus may be used instead, but only in those countries where this procedure is allowed by law.
Gamete donation always reduces the couple’s theoretical risk of having a child affected with a particular disease to a general population risk, that is to a low risk, but never to a 0%. 0 and 100 do not exist in this field, so we always speak in terms of probabilities. Assisted reproduction techniques can be employed in disorders for which there is no prenatal diagnosis, or in disorders for which a prenatal diagnosis does exit, but the couple is against terminating a possible pregnancy or do not want to take the high risk of having an affected child if fertilization is performed with their own gametes. If they do not accept this option they can still adopt a child.

But, a word of cautiousness…
It is clear that this technology is helping many couples to have children, but we must also be aware of the fact that these techniques are not free of risks. Some studies published in medical journals report that in vitro fertilisation and intracytoplasmic sperm injection (ICSI) imply a higher risk (9%) as compared to that of the general population (4.2%) to have children with congenital defects (diseases, malformations, etc.), or the possibility of multiple pregnancies, prematurity (infants born before their due date) and low birth weight (below 2.500gm). Some of these disorders include:
- Chromosomal alterations, mainly in the sex chromosomes.
- Cardiovascular problems.
- Gastrointestinal malformations.
- Urogenital problems.
- Musculoskeletal disorders and,
- Imprinting defects. In simple terms, we know that each progenitor at the time of fertilisation contributes with one element of each pair of chromosomes or “books” so that at the time of fertilisation, when the 23 chromosomes from the mother + the 23 chromosomes from the father unite, an egg or embryo is formed containing 46 chromosomes. Ok, then. We have seen that in these books or chromosomes that contain all our recipes and during this period of chromosomal reduction (that is, cells that only contain 23 develop from cells that contain 46 chromosomes each), known as meiosis, some of the recipes are blocked or inactivated. In other words, the recipe will be expressed or not expressed (a process known as imprinting made throught a DNA methylation ) depending on whether this chromosomal reduction has taken place in the ovary or in the testicle.
We now know of some children being born with Angelman´s syndrome and Beckwith-Wiedemann´s syndrome, as a result of losing this differential expression in the recipes because the egg has been disturbed and is thus “unbalanced”.
- Angelman’s syndrome: Severe mental retardation, microcephalia (small head), intense seizures, abnormal gait, speech deterioration, trembling, inadequate behaviour patterns of happiness manifested by frequent laughing and excitability.
- Beckwith-Wiedemann’s syndrome: Exopthalmos (a protrusion of the eye ball), Macroglosia (increased volume of the tongue), Gigantism (a growth disorder characterised by excessive growth of the body), Omphacele (umbilical hernia), Neonatal hypoglycaemia (decreased levels of blood glucose), Visceromegalia (large internal organs, liver, kidneys, spleen, and suprarenal glands).
7,5% of affected individuals have tumours, with most tumours appearing in the five years of life, including Wilm´s tumour (malignant tumour of the kidney), hepatoblastoma (liver tumour), neuroblastoma (tumour of the central nervous system, and rhabdomyosarcoma (malignant tumour of muscular tissue).
Why these congenital defects develop is not clear, but it could be due to:
- In some cases, we are interfering with the natural selection process that takes place in each pregnancy, facilitating the union of gametes that would have never taken place otherwise.
- The union of the gametes or “fertilisation”, under normal or physiological conditions, occurs in one of the two Fallopian tubes (anatomical structures of the female’s reproductive system or uterine tubes), a very special and well-nourished environment, characterised by a certain temperature, luminescence, oxygenation, and many other unknown parameters that are changed with the employment of these techniques.
What is the situation with ICSI (intracytoplasmic sperm injection)?
Under normal conditions, from all the ejaculated spermatozoa, only one spermatozoon succeeds in penetrating the ovum. From the time the spermatozoon is ejaculated to the time it encounters the ovum that is going to be fertilised, a series of recognition events and cell interactions take place that can lead to a series of changes in the cell and at molecular level of the DNA (deoxyribonucleic acid , or what’s the same, changes in the books that contain our recipes) of the gametes or reproductive cells.
When the ICSI technique is used, this period of recognition and penetration does not exist, for the spermatozoon is introduced directly inside the ovum with the help of a probe needle. Thus, it is highly likely that in some cases these changes do no take place, consequently leading to the appearance of some sort of problem.
To make it simple, when someone rings the door bell, from the time we answer to the time we open the door, we have time to quickly fix our hair, tidy up the place, close the window, etc, but, if instead of ringing the bell, the person walks right in, we have no time to get ready, fix our hair, tidy up the place, or close the window.
Given that hereditary diseases and chromosomal alterations cause costly and long term health problems for the family, such as mental retardation or severe congenital alterations and anomalies, impossible to correct in some cases and prone to correction in others, this situation leads us to the next question.
What is the most prudent course of action in these cases?
It’s very easy.
On one hand, we are aware of the numerous reasons that lead a couple to undergo these techniques. And on the other hand, we know that couples that have undergone an in vitro fertilisation or the ICSI technique run more risk of having congenital defects than the general population.
That is, for as long as we are unable to distinguish between all the couples that undergo these techniques, which run an increased risk of having children with congenital defects, we must be cautious and can elect:
- To inform all the population that is going to undergo any of the assisted reproduction techniques of the risk inherent to the use such techniques.
- To recommend that these pregnancies be controlled with specific studies to rule out these pathologies (ultrasound, foetal chromosomal tests, and specific tests for syndromes that present imprinting alterations or DNA methylation).
- We also recommend that before you undergo any of these techniques, you have a consultation with your geneticist who will evaluate your case and will clarify whatever doubts you may have.
Now, let me introduce you to PubMed, a medical search engine, in case you need to read any of these articles. You may not be familiar with some of the terms that appear in the articles. This is both logical and understandable, but reading through the pages, or just the titles and the summaries or abstracts, will give you an idea of the latest research and data.
Pubmed
PubMed is a database of medical publications compiled by the United States National Library of Medicine that provides access to over 12 million medical references and specialised medical journals since 1960. PubMed is linked to numerous web pages, where you can find complete articles or other information sources.
The official language of this web page and many other pages is English. This is normal because the Internet started in the United States and its use as a commercial and teaching tool has become standard practise for many years.
To obtain information on the area or topic of your interest, you must write the key words in the search window. Given that the official language is English, these key words must be written in English.
These are some of the most commonly used words:
| Search words | |
| Angelman syndrome & ICSI | Search for PubMed results |
| Becwith-Wiedemann syndrome & ICSI & in vitro fertilisation | Search for PubMed results |
| Risk of major birth defects & intracytoplasmic sperm injection & in vitro fertilization | Search for PubMed results |
| In vitro fertilization & human malformations | Search for PubMed results |
| ICSI & human malformations | Search for PubMed results |
| Follow-up of children born after ICSI | Search for PubMed results |
| Prenatal testing in ICSI pregnancies & chromosome anomalies | Search for PubMed results |
| Fertility treatments: Seeds of doubt | Search for PubMed results |
| Intracytoplasmic Sperm Injection May Increase the Risk of Imprinting Defects | Search for PubMed results |
| Infertility Treatment – More Risks and Challenges | Search for PubMed results |
| Low and Very Low Birth Weight in Infants Conceived with Use of Assisted Reproductive Technology | Search for PubMed results |
| Human assisted reproduction technology | Search for PubMed results |
| Human in vitro fertilization | Search for PubMed results |
| Intracytoplasmic sperm injection (ICSI) on human | Search for PubMed results |
| ICSI | Search for PubMed results |
Please be advised that from all the papers found, you must choose those that cover your area of interest. Some of the articles are summarised in the so called “abstracts” and in others only the title is provided with no summary. In some cases, you will be given instructions that will help you find the complete article.
Other alternatives to get the articles are: When you read the article, you will notice that below the authors the title of the article appears followed by the name of the journal in which the article was published, together with the year and corresponding pages. Some articles also provide the e-mail address of the corresponding author.
- You can also visit your local library or other libraries specialised in medicine and biology, or large libraries that cover a wide range of subjects, where the librarian will help you find the material you are looking for so that you can read it there or take it home.
- If you prefer to surf the net, you can go to Free Medical Journals.com a web page that provides free access to numerous medical journals, where you may be able to find the magazine that contains the article at the time of your search. This is because some of the articles are available only on a temporary basis.
You will find that these articles are published in different languages, with English ranking first. Once you have the paper you want, and if you need to have it translated for your convenience, I recommend you enlist the services of a sworn or accredited translator, specialised in medical translation. You can call your Medical Association, Board of Physicians or Biologists or search the net to find the name of a reliable translator.
Next topic: Prenatal Diagnosis techniques
Reviewed: 19th of January 2015