What is heredity and how do we acquire it?

Let’s imagine a mother with her two daughters, who divides her belongings equally between them. The mother has two closets, two chairs, two beds, and she gives each of her daughters: one closet, one chair, one bed, etc.
In our case, what we are dividing is the 23 sets of chromosomes that we have in each of our gonadal cells – that is the cells contained in the ovaries and the testis.
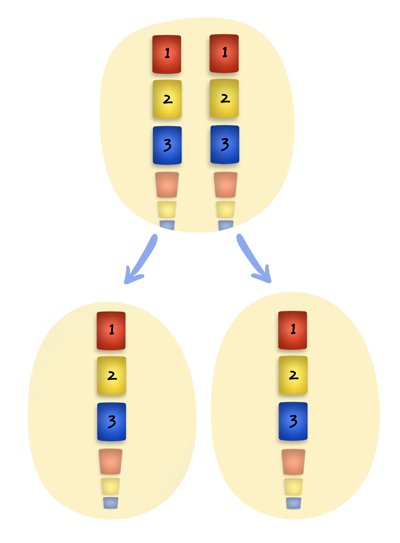
Remember that the parent cell, both in the ovary and in the testis, contains 46 chromosomes arranged into 23 sets before it undergoes cell division. When meiotic division takes places, it divides the chromosomes equally between both daughter cells. Thus, from the two chromosomes contained in set 1, one is given to each daughter cell, and this process is repeated for each of the remaining sets. In the end, each daughter cell will have received 23 chromosomes, or what is the same, an element from each set.
Subsequently, when the ovum and the spermatozoon unite, an individual with 46 chromosomes (23 from the mother + 23 from the father) is obtained. In this manner, the number of chromosomes in the human race is preserved.
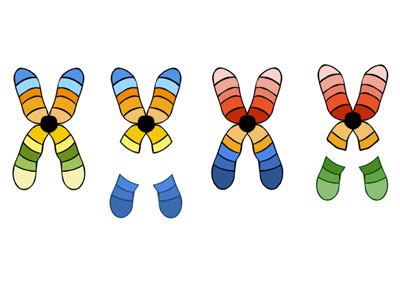
Let’s also note that the information of the recipes contained in the chromosomes is copied twice (with the exception of sex-chromosomes in the male “XY”). From chromosome or cassette number 1, we have two copies: one inherited from the father and one inherited from the mother. Simply because they are from the same cassette number, they must contain exactly the same recipes with exactly the same type of information, but with the specific variables that make up each individual.
Suppose that recipe number 25, inherited from the maternal “cassette” number 2, contains information for blond hair, and that the one we have inherited exactly from the same place, but from the father’s side, is for black hair. Both chromosomes or cassettes are giving us exactly the same information (HAIR COLOR), but with the traits or variables that each individual presents (BLOND hair or BLACK hair).

Consequently, the instructions for hair are received twice. The new individual will on some occasions express the instructions given in both recipes, and on other occasions it will only express one set of instructions, despite having both sets, because one will dominate over the other. That is, it is easier for the dominant set of instructions to express or manifest itself than it is for the other. In our example, the individual will have black hair because black hair dominates over blond hair, but remember that the individual carries both recipes or sets of instructions: black hair and blond hair. This situation is repeated for all recipes over and over again.
Nonetheless, in life anything can go wrong and this is also true for nature.
Concerning our inheritance, these failures can be originated by:
Alteration in the number
That is, the inheritance received by the daughter cells is different between them as a result of an error in the distribution: some daughter cells receive more while others receive less chromosomes. 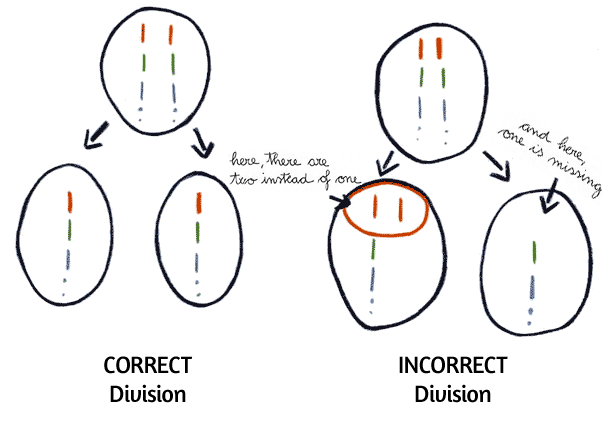
If gametes that have resulted from an erroneous division fertilise the egg, then we will find that the individual at issue will have a greater or lesser number of chromosomes.
For instance,
Children with Down syndrome or trisomy of chromosome 21 are the result of one of the gametes with which they were fertilised, transmitting two instead of one chromosome from set 21. When this gamete united with the gamete from the other progenitor, an egg was “produced” which contained three chromosomes in set 21, instead of the normal two chromosomes.
This would be equivalent to a rice dish to which instead of adding salt twice, we have added salt three times.
So, it will consequently be salty. In our case, and depending on the chromosome involved, one or another type of malformation or malformations will appear.
Alteration in the structure
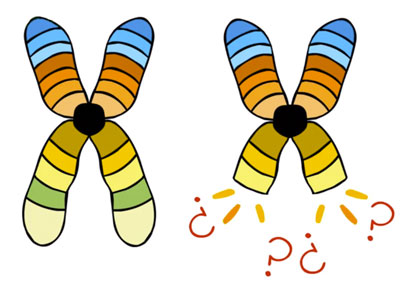
Deletion
In this case, the distribution is correct but some chromosome or cassette was defective because it is missing a tiny part (an alteration known as “deletion”);
Translocation
or this tiny bit had attached to another chromosome;
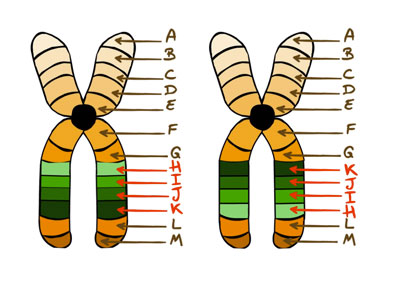
Inversion
Or it had inverted within the same chromosome, giving an erroneous reading sequence, an alteration known as “inversion”), etc.
As you can imagine, theses structural alterations that we just mentioned are the most common, but there are some more different situations, as you will see in further questions.
However, there are many other types of alterations, as you will be able to read in related questions listing. In general, many of these alterations act by mixing the information contained in the recipes involved. This situation may or may not lead to the development of pathologies, depending on where the recipe is torn, inverted or attached. If the recipe has been torn in the middle, the information that it contains will be incomplete, and thus invalidated.
In other cases they can cause defective gametes because during their “fabrication” process they lack or gain a chromosomic fragment.
In other words, in order for everything to be OK, each cell must inherit 23 sets of complete chromosomes or cassettes. Otherwise, if one receives more than the other or the information is mixed, we will run into a series of cell unbalances, which will manifest in a wide variety of disorders such as:
- Miscarriages, as the presence in triplicate of the same chromosome or the absence of a chromosome or one of its portions, can produce such an important unbalance that it makes the foetus or embryo unviable.
- Malformed infants that can die soon after birth, depending on the severity of their malformations.
- Infants that may reach maturity with malformations and/or disability.
Related questions
- What type of chromosomal alterations of a structural origin can occur?
 Look at me! I am a chromosome and many things can happen to me. All the things that can happen to me have different names.
Look at me! I am a chromosome and many things can happen to me. All the things that can happen to me have different names.

I can loose part of my material
If this happens at both extremes, I bend and form what is referred to as a RING CHROMOSOME.

Maybe a bit breaks off and then the detached bit attaches to another chromosome
If a bit from two chromosomes detaches from their extremes and we exchanged that bit, then it is called RECRIPROCAL TRANSLOCATION.
And if instead of just one bit attaching , what attaches to another chromosome is an entire chromosome , as it can occur in chromosomes 13, 14, 15, 21, and 22, then it is called ROBERTSONIAN TRANSLOCATION.
 I can also break in two different parts, turn myself around and attach myself again.
I can also break in two different parts, turn myself around and attach myself again.
If the rupture occurs outside the area of the waist, it is called PARACENTRICAL INVERSION.

Apart from this, at the time of cell division, I can make a mistake and instead of dividing longitudinally, I can do it cross-wise
This is referred to as ISOCHROMOSOME.
 Sometimes during cell division I may loose a small bit that becomes free and which may end up joining another cell that already has all its chromosomes
Sometimes during cell division I may loose a small bit that becomes free and which may end up joining another cell that already has all its chromosomesThis is called MARKER CHROMOSOME.
 I can also increase in size in specific places without causing any type of alteration or pathology because I do at the expense of a neutral material
I can also increase in size in specific places without causing any type of alteration or pathology because I do at the expense of a neutral materialThis can happen to me if I am a type 1, 9, 16 or Y, identifying myself as 1qh+, 9qh+, 16qh+ or Yqh+. Given the frequency of this alteration, geneticists consider it a variant of what is considered normal.

- What is the difference between a child with Down's syndrome caused by a regular trisomy or a Robertsonian translocation?The clinical picture is the same because Down’s syndrome occurs when the given individual has three chromosomes from pair 21 instead of the normal two. What happens is that in a regular trisomy, the three chromosomes from pair 21 are separated whereas in a Robertosian translocation two are separated and the other one fused with another chromosome.However, the difference between the two types is found in the risk of repetition in future pregnancies.
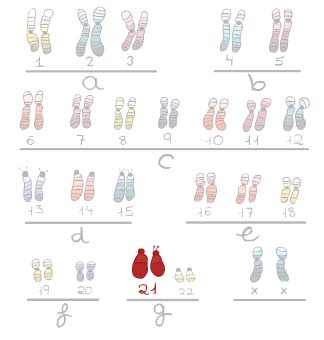
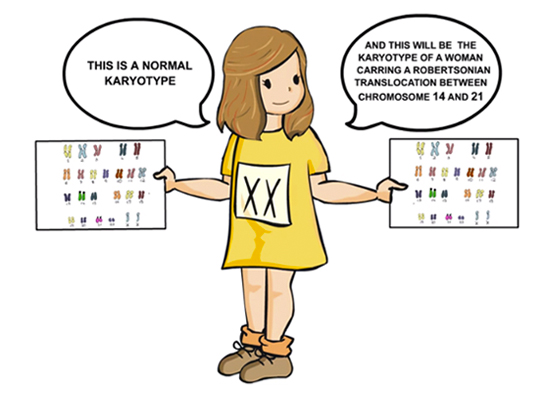
Normal Karyotype: it only has 2 chromosomes from pair 21. 
Pathological karyotype: It has 3 chromosomes from pair 21 (Trisomy from pair 21) = Down’s syndrome caused by regular trisomy. 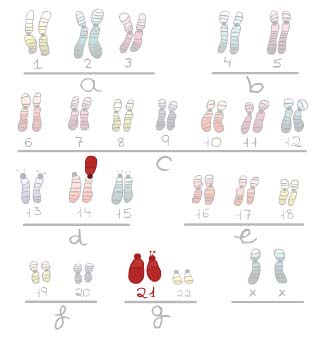
Pathological karyotype: It has 3 chromosomes from pair 21, (two are separated and one trasnlocated or fused with a 14 chromosome). In this case, we will have a case of Down’s syndrome caused by a Robertsonian translocation. Risk for Regular Trisomy
For the general population, the probability to have a child with Down syndrome due to a regular trisomy basically depends on the maternal age and on the stage the pregnancy I at (in terms of weeks of gestation). That is, the more advanced the pregnancy the lower the risk because many of the affected foetuses are spontaneously aborted or diagnosed prenatally. Below, please find a table indicating the risk based on a study published by Cuckle, Wald and Thomson in 1987. Please notice that the table presents two possibilities broken-down into years:
- The possibility to have a child with Down Syndrome during the second trimester screening (15-20 weeks).
- The possibility to have a child with Down Syndrome in a full term pregnancy, that is, at birth.
If a woman aged under 35 has had a child with Down’s syndrome, the risk of repetition in a future pregnancy is 1 in 100 – 1 in 200. From this age onwards, the risk is practically the same as that of the general population.
Let’s review what meiosis is:
View male Meiosis animation View female Meiosis animation
Let’s see at a case of meiosis that will result in Down’s syndrome caused by regular trisomy.
Risk of Robertsonian Translocation
If on the contrary the Robertsonian translocation is between chromosome 21 and any of the acrocentric chromosomes 13, 14, 15, 21 or 22, two situations can arise:
- That the translocation manifests itself for the first time in the affected child, thus the repetition risk is very low because paternal gonadal mosaicism cannot be ruled out, or
- That one of the parents has the balanced Robertsonian translocation; if this is the case, the repetition risk in a future pregnancy will depend on the involved chromosomes and the gender of the progenitor carrying the translocation.
The repetition risks if the translocation occurs between chromosomes 13 and 14, or 15 and 21, are:
- If the mother is the carrier, the risk is between 10-11%
- If the father is the carrier, the risk is about 2,4%
- If the mother is the carrier, the risk is 14%
- If the father is the carrier, the risk is 1-2%
Let’s review what a Robertsonian translocation is:
Let’s review what meiosis is:
View male Meiosis animation View female Meiosis animation
Let’s see what happens during meiosis when one progenitor is the carrier of a Robertsonian translocation between chromosome 14 and 21.
And lastly, a special case:
Should the Robertsonian translocation occur between two chromosomes of pair 21 of one of the progenitors, the expected offspring would all suffer from Down’s syndrome or have miscarriages.
In this case, the repetition risk is 100%.




Chromosomal alterations with regards to the information contained in the chromosome
In this case, the transmission of chromosomes is correct, both in number and in structure, since we have inherited all the chromosomes or cassettes, with all the recipes included. However, part of the information in one of the recipes is incorrect. For instance, if we follow a recipe to bake a cake, but in the ingredients, instead of sugar they tell us to use salt, the result would be an inedible cake. This, applied to our recipes, would be a malformed or dysfunctional organ. Given that our body has formed from instructions provided by different recipes, any of them may be defective. Consequently, any part or function of our body may be affected with a malformation, anomaly or dysfunction.
And, how do these defects, malformations or deficiencies behave?
Some are very severe, and those individuals who are affected with the condition die before they reach their reproductive age. Other individuals may reach their reproductive age, but their disorder incapacitates them and they cannot reproduce, and thus, they cannot transmit the disorder to their descendants. Others, have the disorder or deficiency and can reproduce and transmit it to their children. It is also possible for a given individual at the time of reproduction to have a disorder that has not yet manifested. If there is no family past history suggesting this possibility, the first symptoms may appear when reproduction has already taken place, and thus it may be too late to put some sort of prevention into place. Should that be the case, the individual may have already transmitted the disorder to the offspring.  This works in the same way as an alarm clock that has been set to go off at a certain time. In our case, the disorder or dysfunction may have been programmed at the time of conception.
This works in the same way as an alarm clock that has been set to go off at a certain time. In our case, the disorder or dysfunction may have been programmed at the time of conception.
And, what can be done in a case of malformation or deficiency?
The malformation or deficiency has to be studied in all cases and the risk of the couple to have a child affected with the same malformation assessed. If this assessment indicates that some risk exists, the different possibilities available to us have to be evaluated in an attempt to prevent it. These possibilities include specific prenatal diagnosis, which should be conducted in the early stages of pregnancy, should the option to voluntarily terminate the pregnancy be called for. Or, if the woman does not wish to terminate her pregnancy, prenatal diagnosis enables us to plan the most adequate course of action for the actual delivery (that is vaginal delivery or C-section), and to choose the type of treatment to follow before and after the birth in order to reduce to a minimum the disorder or lesions and thus succeed in achieving a better quality of life. Another option in these cases is to assess the possibility of employing assisted reproduction techniques, such as sperm or human ovocyte donation, or a preimplantational diagnosis in cases where the couple does not accept termination of the pregnancy due to their religious beliefs or philosophy of life, thereby avoiding the birth of an affected child from a future gestation. In some cases there is no family past history of malformations or deficiencies, but still, infants are born with problems.
So, why does this happen?
It happens because there are two large groups of malformations and/or deficiencies:
- hereditary malformations and/or deficiencies
- and environmental malformations and/or deficiencies
a) Hereditary malformations and/or deficiencies present a known repetition risk in future pregnancies which can be assessed beforehand, b) whereas environmental malformations and/or deficiencies are accidental and their recurrence is very unlikely.
The problem here is to find out whether a malformation that appears for the first time in a family has a hereditary component or if, on the contrary, it is environmentally related. In other words, a child can suffer a cardiac malformation because either he or she has received the wrong “recipe” and, consequently, his or her malformation is hereditary, or because his or her mother accidentally took a medication or had an infection while she was pregnant with the child, and such medication or infection interfered at the time when the heart was being formed, leading to a malformation that, in this particular case, is environmentally and not-hereditarily related. This explains why a pregnant woman should never take any medications without her physician’s consent. Throughout the course of our lives, our hereditary material is subjected to many changes. The problems, malformations, deficiencies or disorders only appear when the changes that affect our “recipes” are unfavourable. Nevertheless, in the majority of cases, these are neutral changes that have no repercussion, or favourable changes that help us adapt and survive in the environment in which we live. Let’s suppose that a couple, with a normal IQ, is considering starting a family and that in the gametes of either prospective parent, a change or mutation takes place in one of the many genes or “recipes” that encode intelligence. This change or mutation can lead to three possible scenarios:
- that the unborn child has a normal intelligence like his or her progenitors
- that the child is a genius
- that the child is mentally retarded
- Perhaps the car had a production fault, caused by an error in one of the assembly lines, and therefore, all cars that went on that assembly line will encounter the same fault. In our analogy, this would be equivalent to a child with a hereditary defect or malformation.
- In contrast, it is possible that the car does not have any manufacturing problem. It is simply a flat tire that caused the accident, or an accidental event at a given time.
On the other hand
During child development, all body organs grow simultaneously but specifically, with the different recipes necessary for their formation expressing in each organ, respectively. Sometimes there are some recipes or components that are essential for the formation of many organs and, in these cases, the recipes or components are shared by several of these organs simultaneously. Here’s another analogy; salt in the kitchen. Salt is used in a variety of dishes but if the salt has gone wrong, then many dishes will be spoiled. Within the complexity of our organs, a great many use the same recipe to build their different structures, and if this recipe is altered, many organs will be affected. The severity of the malformation will depend on the percentage in which the defective recipe was used, specifically within each organ. Some recipes take a lot of salt while others take less salt. So, if a recipe is incorrect, and it is used in one single organ, this organ, may individually present a malformation. However, if the same recipe is used in several organs simultaneously, then several organs will be malformed. In all cases, the degree of severity will depend on the percentage in which the defective recipe was used, and also on the influence from the other recipes being expressed jointly in each organ at the same time, which modifies the expressivity degree of the defective recipe. A cake is not the result of one single ingredient. The final taste will depend on the contribution or mix of all its different ingredients. Therefore, all these recipes are out there doing their job and all human beings have good and bad recipes. An individual will be the result of mixing up all these recipes. And, it is this combination of good and bad what makes us unique and unrepeatable beings, with a determined heredity and a special susceptibility for everything that surrounds us. 
And so, what is heredity?
Heredity is a set of chromosomes with their recipes that we have received or inherited from our parents and which we will pass on to our own children.
As we mentioned before, chromosomes are classified in 23 sets. The first 22 sets are called AUTOSOMES and are the same in the man and in the woman. The components of set 23 are called GONOSOMES, or sex-chromosomes, and they are different in the man and in the woman. As their name indicates, they determine the sex of the human being. A woman has two sex-chromosomes “XX” while a man has one “X” chromosome and one “Y” chromosome.
Next topic: Types of inheritance
Reviewed: 22nd of November 2014